CPT Code 83036: Hemoglobin A1c Billing, Medicaid Coverage & Medical Billing in the USA
If you’ve ever looked at a medical bill or a lab requisition form, you’ve probably seen a string of numbers that look like secret codes. One of the most common—and most important—is CPT code 83036.
It sounds technical, but stick with me. This little code represents a test that changes lives: the Hemoglobin A1c test for diabetes management. And whether you’re a patient, a doctor’s office manager, or a medical biller in the USA, understanding CPT 83036 can save you time, money, and a whole lot of confusion.
In this guide, we’ll walk through everything:
- What the test is (in plain English)
- How billing works with Medicaid and private insurers
- Real-world medical billing in the USA pitfalls
- Tips to get claims paid the first time
Let’s dive in—no medical degree required.
What Exactly Is CPT Code 83036? (No Jargon, Promise)
CPT code 83036 stands for:
Hemoglobin; glycosylated (A1c), by a laboratory method using chromatography or immunoassay.
Translated: It’s a blood test that measures your average blood sugar over the past 2 to 3 months. Unlike a daily finger prick, this test looks at the big picture.
Doctors use it to:
- Diagnose prediabetes and type 2 diabetes
- Monitor how well diabetes treatment is working
- Adjust medications like insulin or metformin
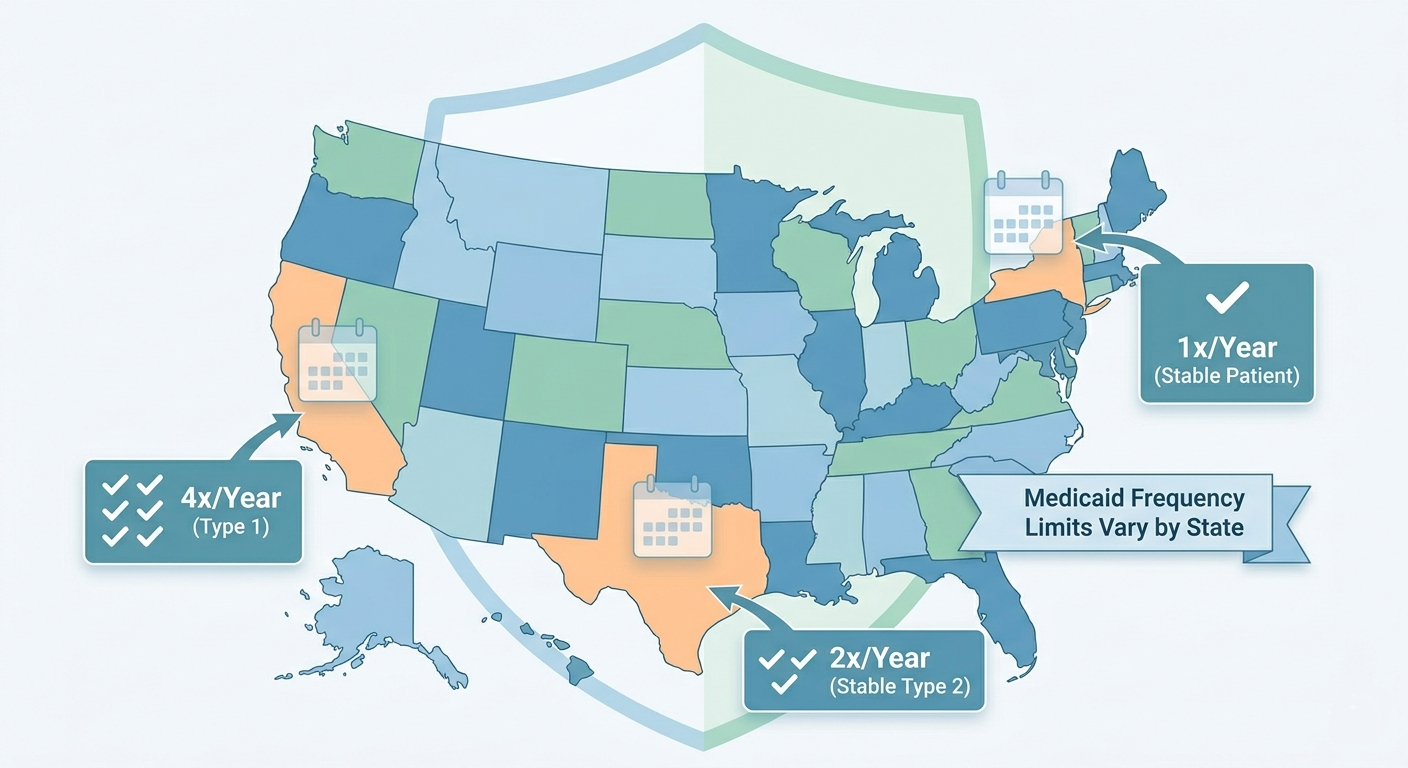
The test is usually done 2 to 4 times a year for people with diabetes. For stable patients, once a year might be enough.
Why “83036” Matters in Medical Billing in the USA
In the messy, wonderful world of medical billing in the USA, every service gets a code. 83036 is the specific code for lab-based A1c testing.
There’s also CPT 83037 (point-of-care A1c, done in the doctor’s office with a small device), but 83036 is for a lab. Why does that matter? Reimbursement rates differ, and some payers (including many Medicaid plans) prefer the lab version.
Knowing the difference is the difference between getting paid and getting a denial.
Medicaid and CPT Code 83036: What You Need to Know
Medicaid covers A1c testing, but each state runs its own program. That means coverage rules for CPT 83036 can vary if you’re in Texas, California, New York, or Florida. However, some things are universal.
Does Medicaid Cover CPT 83036?
Yes—almost always. The test is considered medically necessary for:
- Patients with a diagnosis of diabetes (E08-E13 in ICD-10)
- Patients with gestational diabetes
- Patients with prediabetes (once every 12 months in many states)
But here’s the rub: Medicaid may limit frequency. Common limits:
- Up to 2 tests per year for stable type 2 diabetes
- Up to 4 tests per year for type 1 diabetes or unstable glucose control
- More frequent testing requires prior authorization or medical records showing a change in therapy
Medicaid Billing Tips for CPT 83036
If you’re a billing specialist or a small clinic owner, these steps save denials:
- Verify eligibility before the patient leaves the waiting room. Many Medicaid plans are managed by private insurers (e.g., Medicaid MCOs).
- Use the correct diagnosis code. For diabetes, use the specific ICD-10 code (e.g., E11.9 for type 2 without complications). For prediabetes, use R73.03.
- Modifier alert– Most labs don’t need modifiers for 83036, but some state Medicaid programs require QW (CLIA-waived test) if done in a physician’s office lab. Check your state’s provider manual.
- Place of service (POS) POS 81 (independent lab) vs. POS 11 (office) can change reimbursement.
Real-life example: A small family practice in Ohio billed 83036 with POS 11 for a Medicaid patient. Denied. Reason? Their state Medicaid required POS 81 for lab codes unless the office had a specific lab certification. A simple fix—but it cost them 45 days in accounts receivable.
Medicaid Reimbursement Rates for 83036
Rates vary wildly. For example:
- California Medicaid (Medi-Cal): ~$8–$12 per test
- New York Medicaid: ~$6–$10
- Texas Medicaid: ~$7–$11
Private insurance pays more (often $15–$30), but Medicaid keeps the lights on for many community health centers. The key is volume and clean claims.
The Human Side of Medical Billing in the USA (With CPT 83036)
Let’s be honest: Medical billing in the USA can feel like a trap designed to frustrate everyone. Patients get surprise bills. Billers get endless denials. Doctors get paid months late.
But when it works, CPT 83036 is a quiet hero.
Imagine a 58-year-old grandmother named Rosa. She has type 2 diabetes and sees her doctor every 3 months. Her A1c result? 8.5% (goal is under 7%). The doctor increases her medication. Three months later, a repeat 83036 shows 7.2%.
That code—just five digits—helped Rosa avoid kidney damage, blindness, and neuropathy.
Medical billing in the USA isn’t just about money. It’s about making sure Rosa’s test gets run, her doctor gets paid fairly, and Medicaid (or her private plan) covers it without a fight.
Common Denials for CPT Code 83036 and How to Fix Them
Even with a simple lab test, denials happen. Here’s what to watch for:
| Denial Codes | Reason | Fix |
| CO 50 | Not medically necessary (too frequent) | Check date of last A1c; appeal with medical records showing change in meds |
| CO 97 | Benefit for this service is not included in patient’s plan | Some Medicaid plans exclude routine diabetes monitoring? Rare, but verify benefits |
| PR 204 | Service not covered by this payer | Ensure you’re billing the correct Medicaid MCO, not the state directly |
| CO 151 | Payment adjusted because payer deems frequency exceeds medical necessity | Appeal with documentation of unstable diabetes |
Pro tip: Always document the medical necessity in the patient’s chart. “Diabetes, uncontrolled” is vague. Instead: “Type 2 diabetes with recent insulin initiation, requiring A1c to guide dose changes.”
CPT 83036 vs. 83037: Which One Should You Bill?
This is a huge source of errors in medical billing in the USA.
- 83036= Lab-based A1c (send blood to an outside lab or your in-house certified lab)
- 83037= Point-of-care (POC) A1c (small device in the exam room, results in minutes)

Payer Preferences
| Payer | Prefers 83036 | Prefers 83037 | Notes |
| Medicare | ✔️ | ❌ | Medicare covers 83037 only in certain settings (e.g., rural) |
| Most Medicaid | ✔️ | Sometimes | Many state Medicaid plans require 83036 for reimbursement |
| Private insurers | Depends | Depends | UnitedHealthcare often covers both; Aetna may require prior auth for POC |
Why does it matter?
If you use a POC device but bill 83036, that’s a misrepresentation. If you bill 83037 for a lab test, same problem. Auditors love this one.
Can You Bill Both on the Same Day?
Generally, no. Medical billing guidelines (including those from the AMA and CMS) say you should not bill 83036 and 83037 for the same patient on the same date of service unless there’s a very specific medical reason (e.g., a lab error). Doing so looks like fraud.
Step-by-Step: How to Bill CPT Code 83036 for Medicaid (And Get Paid)
Let’s walk through a real-world medical billing in the USA scenario.
Patient: Juan, 45, Texas Medicaid (Molina plan)
Service: A1c lab drawn in your office, sent to Quest Diagnostics
Frequency: Last A1c was 4 months ago; doctor needs a new one to check metformin effectiveness.
Step 1 – Check eligibility
Log into Molina’s portal or use your clearinghouse. Confirm active coverage and that A1c testing is a covered benefit (it almost always is).
Step 2 – Collect diagnosis
ICD-10: E11.9 (Type 2 diabetes without complications) – this works for routine monitoring.
Step 3 – Complete the claim form (CMS-1500)
- Box 24D: 83036
- Box 24E: One unit (unless you’re doing a rare repeat same day – don’t)
- Box 21: E11.9
- Box 24F: $ charge (your lab’s contracted rate – for Medicaid, it’s usually a state fee schedule)
- Box 33: Your billing NPI
Step 4 – Submit electronically
Most billers use a clearinghouse like Office Ally, Change Healthcare, or Waystar. Texas Medicaid accepts direct submission via TMHP.
Step 5 – Follow up
If not paid in 30 days, check the remittance advice. Common Texas Medicaid edits for 83036:
- Edit 0477 – “Services not covered unless performed in an independent laboratory” → Appeal with your CLIA certificate if you have an in-house lab.
- Edit 0469 – “Frequency exceeds medical necessity” → Send medical records.
Juan’s claim result: Paid $8.43 in 22 days. Not a fortune, but clean and predictable.
Why Medical Billing in the USA Feels Broken (But Can Work for CPT 83036)
I’ve talked to billers who cry at their desks. I’ve talked to patients who got a $200 bill for an A1c that should have cost $10. I’ve talked to doctors who say they’d rather treat patients than fight with insurers.
But here’s the truth: CPT code 83036 is one of the easier codes to master. It’s well-defined, widely covered, and rarely denied if you follow the rules.
The hard part is keeping up with state Medicaid changes. In 2025 alone:
- Florida Medicaid changed its A1c frequency limit from 4 to 2 per year for non-insulin patients.
- California added a requirement for a diabetes diagnosis code in the first position.
- New York started denying 83036 when billed with routine physicals (use Z00.00 at your own risk).
Solution: Join a local medical billing association (like HBMA or your state’s MGMA chapter). Subscribe to Medicaid updates via email. And never assume last year’s rules apply this year.
Frequently Asked Questions (From Patients and Billers)
Q: Can a patient be billed for CPT 83036 if Medicaid denies it?
A: In most states, Medicaid beneficiaries cannot be balance-billed for covered services. If Medicaid denies, you must appeal or write it off (unless the patient signed an ABN – Advance Beneficiary Notice – before the test).
Q: How often can I bill CPT 83036 for a Medicaid patient with type 1 diabetes?
A: Usually up to 4 times per year. Some states allow 6 if the patient is pregnant or has recent hospitalizations. Check your state’s fee schedule.
Q: Is CPT 83036 covered for prediabetes?
A: Yes, but usually only once every 12 months. The diagnosis code is R73.03. Some Medicaid plans require prior authorization for this use case.
Q: What’s the difference between CPT 83036 and 83036-59?
A: Modifier 59 (distinct procedural service) is rarely needed for A1c unless you’re doing another lab test that normally bundles. Just leave it off unless a payer instructs otherwise.
Q: Do I need a CLIA number to bill CPT 83036?
A: If you draw the blood and send it to a lab, no. If you run the test in your office (even a POC device), yes – you need a CLIA certificate. Medicaid won’t pay without it.
Checklist: Before You Hit “Submit” on Your 83036 Claim
[ ] Patient’s Medicaid active?
[ ] Last A1c date documented? (to avoid frequency denial)
[ ] Correct ICD-10 (E11.x, E10.x, R73.03, etc.)?
[ ] POS code matches where service was performed?
[ ] No duplicate billing of 83036 and 83037?
[ ] CLIA number on file (if in-house testing)?
[ ] State-specific prior authorization (rare but check)?
Do these seven things, and you’ll join the top tier of medical billing in the USA professionals who actually enjoy Mondays.
CPT Code 83036 Is a Small Number With a Big Job
Whether you’re a patient trying to understand a bill, a medical assistant learning the ropes, or a biller handling hundreds of claims a day—CPT code 83036 represents something: the quiet, everyday work of managing a chronic disease that affects 38 million Americans.
Medicaid ensures that low-income patients get this life-saving test. Medical billing in the USA ensures that labs and doctors can stay open to provide it.
Next time you see 83036 on a claim form, you’ll know: it’s not just a code. It’s a check-in. A course correction. Sometimes, it’s a second chance.
And now you know exactly how to bill it, appeal it, and get it paid.