If your practice prescribes semaglutide, tirzepatide, or any GLP-1 receptor agonist, you already know the clinical demand has never been higher. What you may not fully appreciate is how quickly GLP-1 medical billing errors are quietly draining your revenue — especially in weight loss drug billing, where payer criteria shift constantly and documentation gaps are easy to miss. Denial rates for specialty drug claims — including GLP-1 medications — have climbed to some of the highest levels seen in outpatient billing history. For a practice managing dozens of GLP-1 prescriptions per month, even a modest denial rate translates to thousands of dollars in delayed or permanently lost reimbursement.
At Utreatibill, our Revenue Cycle Management Services are built specifically to handle the complexity that comes with GLP-1 drug billing 2026 — from the right code combinations to payer-specific prior authorization workflows that actually get approved. This guide covers everything your practice needs to stop losing money on GLP-1 claims.
What Is GLP-1 Medical Billing?
GLP-1 medical billing refers to the complete process of coding, submitting, and securing reimbursement for GLP-1 receptor agonist medications — including Ozempic, Wegovy, Mounjaro, and Zepbound — from Medicare, Medicaid, and commercial payers. It requires accurate ICD-10 diagnosis codes, correct HCPCS or NDC codes, prior authorization documentation, and payer-specific compliance to avoid claim denials.
What Is GLP-1 Medical Billing in 2026?
GLP-1 medical billing covers the full reimbursement cycle for a class of injectable medications that have become central to treating type 2 diabetes, obesity, and cardiovascular disease. The drugs in this class — semaglutide (Ozempic, Wegovy, Rybelsus), tirzepatide (Mounjaro, Zepbound), liraglutide (Victoza, Saxenda), and dulaglutide (Trulicity) — are among the most prescribed and most expensive outpatient drugs in the country.
Billing for these medications is not straightforward. The distinction between GLP-1 for type 2 diabetes vs. obesity billing is where most practices first encounter confusion — because the rules vary depending on the clinical indication, the payer type (Medicare vs. commercial vs. Medicaid), the benefit pathway (medical benefit vs. pharmacy benefit), and the dispensing setting (specialty pharmacy vs. in-office administration). Getting any single element wrong results in a denial — and that denial costs your practice time, staff resources, and real money.
Why GLP-1 Medical Billing Has Become a Revenue Priority for Every Practice
What Changed in GLP-1 Coverage After Recent CMS and Payer Policy Shifts
The GLP-1 reimbursement landscape shifted significantly in 2024 and 2025. CMS expanded its approach to GLP-1 coverage for cardiovascular risk reduction following FDA approvals for semaglutide in that indication. Commercial payers responded with revised formulary tiers, updated prior authorization criteria, and tighter step therapy requirements. What was approved under one set of rules in 2023 may now require different documentation, a different diagnosis code combination, or an entirely new step therapy pathway.
CMS GLP-1 Coverage Extensions and What’s Permanent in 2026
As of 2026, CMS confirms that Medicare Part D covers GLP-1 medications approved for type 2 diabetes management when prescribed within FDA-approved labeling. Coverage for obesity-only prescribing remains restricted under traditional Medicare, though select Medicare Advantage plans have begun offering enhanced GLP-1 formulary access for weight loss indications. The 2026 physician fee schedule also introduced updated HCPCS guidance and drug billing clarifications for high-cost specialty claims.
Why Many Practices Are Still Leaving GLP-1 Reimbursement on the Table
Most practices are not losing GLP-1 revenue because they are prescribing incorrectly. They are losing it because their billing workflows have not kept pace with payer policy changes. The most common issues include submitting claims with outdated ICD-10 codes, failing to include sufficient step therapy documentation in prior auth packets, and routing claims through the wrong benefit pathway entirely.
The Hidden Revenue Risk of Incorrect GLP-1 Drug Billing
A single denied GLP-1 claim can represent $800 to $1,200 in lost monthly revenue per patient. Multiply that across 30 or 40 GLP-1 patients, and an under-performing billing workflow becomes a serious financial problem — fast. Ozempic billing and reimbursement errors are not edge cases, and neither are weight loss drug billing mistakes tied to Wegovy and Zepbound — both of which carry stricter payer scrutiny than their diabetes-indication counterparts. For many practices in 2026, GLP-1 billing gaps represent the largest source of uncollected revenue on the books.
The Financial Cost of GLP-1 Billing Errors in 2026
The data on GLP-1 billing tells a clear and urgent story:
- GLP-1 prescriptions grew by more than 200% between 2021 and 2024, driving an explosion in associated billing volume across primary care, endocrinology, and obesity medicine specialties.
- According to AMA physician survey research, 93% of physicians report that prior authorization requirements delay patient access to necessary medications — with GLP-1 drugs among the most commonly affected therapeutic classes.
- The average cost to rework a denied specialty drug claim — including staff time, chart pulls, and appeals preparation — ranges from $25 to $118 per claim, according to MGMA benchmarking data on high-cost drug reimbursement workflows.
- Medicare Advantage plans deny GLP-1 claims at significantly higher rates than traditional Medicare, with some MA plans maintaining non-formulary status for obesity-indication GLP-1 medications entirely.
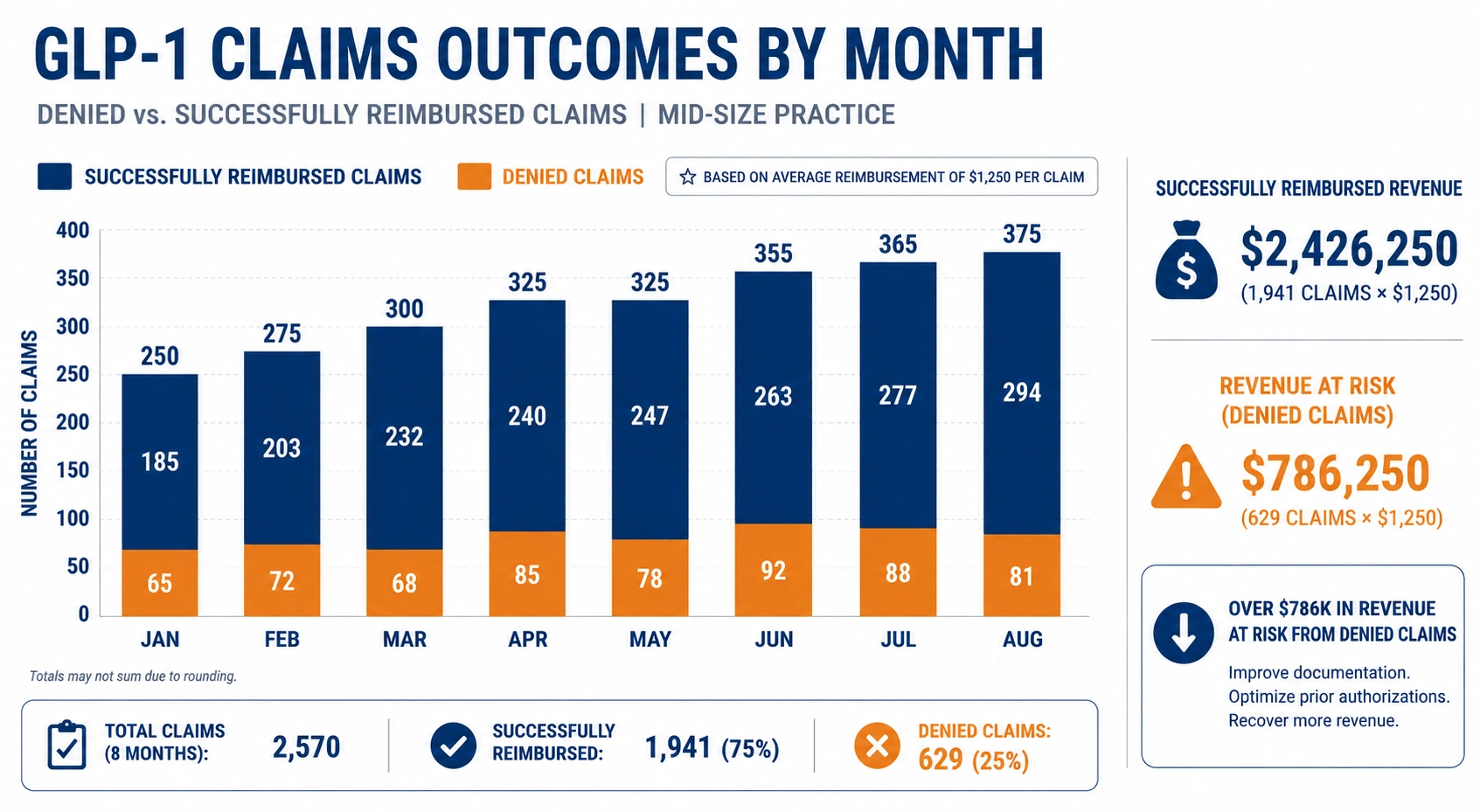
- Industry estimates indicate that practices with no dedicated GLP-1 billing workflow successfully collect on fewer than 70% of submitted GLP-1 claims on the first pass — leaving 30% of revenue stuck in denial and rework cycles.
For a mid-size primary care or endocrinology practice, the gap between GLP-1 prescribing volume and successful reimbursement represents a five- or six-figure annual revenue problem hiding in plain sight.
The Biggest Causes of GLP-1 Billing Denials in 2026
Missing or Incomplete Prior Authorization for GLP-1 Drugs
Prior authorization for GLP-1 is required by virtually every major commercial payer and most Medicare Advantage plans. Submitting a claim without confirmed prior auth — or with an authorization obtained under a different indication — is the single most common cause of denial in GLP-1 insurance coverage claims. The fix is procedural: verify authorization status before the prescription is filled, not after the claim bounces. Understanding GLP-1 prior authorization requirements by payer in 2026 — and building your intake workflow around them — is no longer optional for practices that want consistent reimbursement.
Wrong ICD-10 Diagnosis Codes — Diabetes vs. Obesity vs. Cardiovascular Risk
Payers draw sharp distinctions between GLP-1 prescriptions written for type 2 diabetes (E11.x), obesity (E66.x), and cardiovascular risk reduction. The difference between GLP-1 for type 2 diabetes vs. obesity billing is not just clinical — it determines which diagnosis codes are required, which documentation must accompany the claim, and which payer criteria apply. Using the wrong primary diagnosis code — or omitting a secondary diagnosis that supports medical necessity — triggers automatic denials across most payer systems. ICD-10 code selection must align with both the FDA-approved indication and the payer’s specific clinical criteria for that indication.
Medicare Part D vs. Part B GLP-1 Billing Confusion
Most GLP-1 medications are billed under Medicare Part D as outpatient pharmacy drugs. Part B billing applies only in rare clinical circumstances, such as when a drug is administered in a physician office setting and meets specific incident-to criteria. Confusing these pathways — even inadvertently — produces rejections that are difficult and time-consuming to reverse.
Documentation Gaps That Trigger Automatic Denials
Payers increasingly use automated review logic to flag GLP-1 claims that lack clinical documentation of BMI measurements, HbA1c levels, documented comorbidities, or records confirming that first-line therapies were tried and failed. A missing lab value or absent BMI notation is enough to trigger an auto-denial on some payer systems.
Confusing HCPCS J-Codes With NDC Billing for GLP-1 Medications
When billing under the medical benefit, the correct HCPCS J-code or NDC code must match the specific drug, formulation, and dosage dispensed. Using a J-code associated with Ozempic when Wegovy was dispensed — even though both contain semaglutide — produces a mismatch denial that requires manual correction and resubmission.
Step Therapy and Formulary Restriction Violations by Payer
Most commercial payers require evidence that patients have tried and failed at least one or two prior diabetes or weight management medications before approving GLP-1 drug coverage. Submitting without complete step therapy documentation is among the fastest paths to a systematic denial pattern across your GLP-1 patient population.
The Complete Coding Guide for GLP-1 Medical Billing
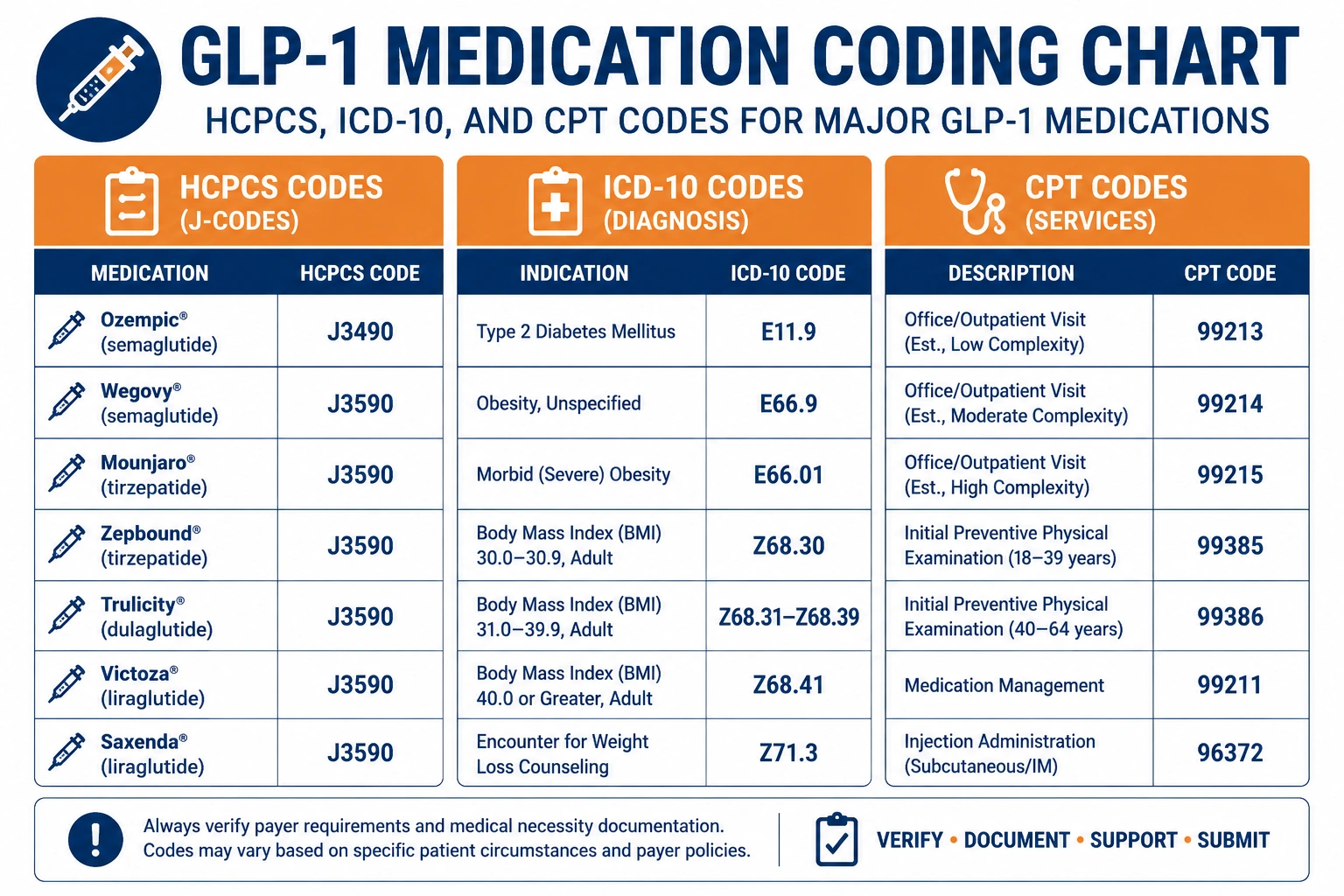
HCPCS and J-Codes for Ozempic, Wegovy, Mounjaro, and Zepbound
| Medication | Generic Name | HCPCS / J-Code | Primary Indication |
|---|---|---|---|
| Ozempic | Semaglutide | J3490 (NOC) / J0604 | Type 2 Diabetes |
| Wegovy | Semaglutide | J3490 (NOC) | Obesity / Weight Management |
| Mounjaro | Tirzepatide | J3490 (NOC) / J0606 | Type 2 Diabetes |
| Zepbound | Tirzepatide | J3490 (NOC) | Obesity / Weight Management |
| Victoza | Liraglutide | J1786 | Type 2 Diabetes |
| Trulicity | Dulaglutide | J0604 | Type 2 Diabetes |
J-codes are updated annually. Always verify current HCPCS codes through CMS and your payer fee schedules before submitting GLP-1 claims.
ICD-10 Codes That Support Medical Necessity for GLP-1 Prescribing
Diagnosis codes on your claim must align precisely with the FDA-approved indication and the payer’s clinical criteria for approval:
- E11.65 — Type 2 diabetes mellitus with hyperglycemia (most commonly required for Ozempic and Mounjaro diabetes claims)
- E66.01 — Morbid (severe) obesity due to excess calories (used for Wegovy and Zepbound obesity claims)
- E66.09 — Other obesity (when BMI supports the diagnosis but does not meet morbid threshold)
- Z68.x — BMI documentation codes (required by most payers as a supporting secondary code)
- I25.10 — Atherosclerotic heart disease (supports cardiovascular indication for semaglutide)
CPT Codes for Office Visits and Counseling Paired With GLP-1 Prescriptions
When billing office visits alongside GLP-1 prescriptions, the E/M code selected must reflect the medical decision-making complexity documented in the note. CPT 99214 and 99215 are commonly appropriate for established patients on GLP-1 therapy given the chronic disease management complexity involved. Obesity counseling codes (CPT 99401–99404) can be billed separately in appropriate clinical scenarios.
NDC Billing for GLP-1 Drugs Under the Medical vs. Pharmacy Benefit
Under the pharmacy benefit, GLP-1 medications are billed using the NDC code through the specialty pharmacy. Under the medical benefit — applicable in limited settings — the 11-digit NDC code must appear on the claim in the correct format, paired with the appropriate unit of measure. NDC formatting errors produce rejections that are rarely flagged with clear explanations, making them difficult to catch and correct quickly.
How Much Revenue Is Your Practice Losing to GLP-1 Billing Errors?
Example 1 — Wrong Diagnosis Code Leads to a Blanket Prior Auth Denial
A primary care practice submits prior authorization requests for 15 Ozempic patients using E11.9 (type 2 diabetes, unspecified) as the sole diagnosis code. The payer requires E11.65 with a documented HbA1c above 7.0% to approve GLP-1 therapy for this indication. All 15 requests are denied. Reworking those 15 prior auth submissions — pulling charts, correcting codes, resubmitting with updated documentation — costs the practice approximately $1,500–$1,800 in staff time before a dollar of revenue is recovered.
Example 2 — GLP-1 Claims Denied for Incomplete Step Therapy Documentation
An obesity medicine practice submits claims for Wegovy across 10 new patients. Each patient is beginning weight management pharmacotherapy for the first time. The payer requires documented evidence of prior failure on at least one FDA-approved weight loss medication or a 6-month supervised lifestyle intervention. Because the prior auth packets do not include this step therapy documentation, all 10 claims are denied. Revenue at risk: $9,000–$12,000 per month — recurring until the workflow is corrected. This is one of the most preventable and most expensive patterns in weight loss drug billing.
Example 3 — Specialty-Specific GLP-1 Reimbursement Gaps in Endocrinology
An endocrinology group bills for Mounjaro using the J3490 NOC code without the required invoice documentation or NDC attachment required by their payer. The payer auto-denies all claims flagged for incomplete documentation. The group does not identify the issue until a monthly Billing Reporting and Analytics review reveals a consistent write-off pattern in the GLP-1 line — a pattern that had been running for three billing cycles before anyone caught it.
Medicare vs. Commercial Payer GLP-1 Rules: A 2026 Comparison
How Does Medicare Cover GLP-1 Weight Loss Drugs?
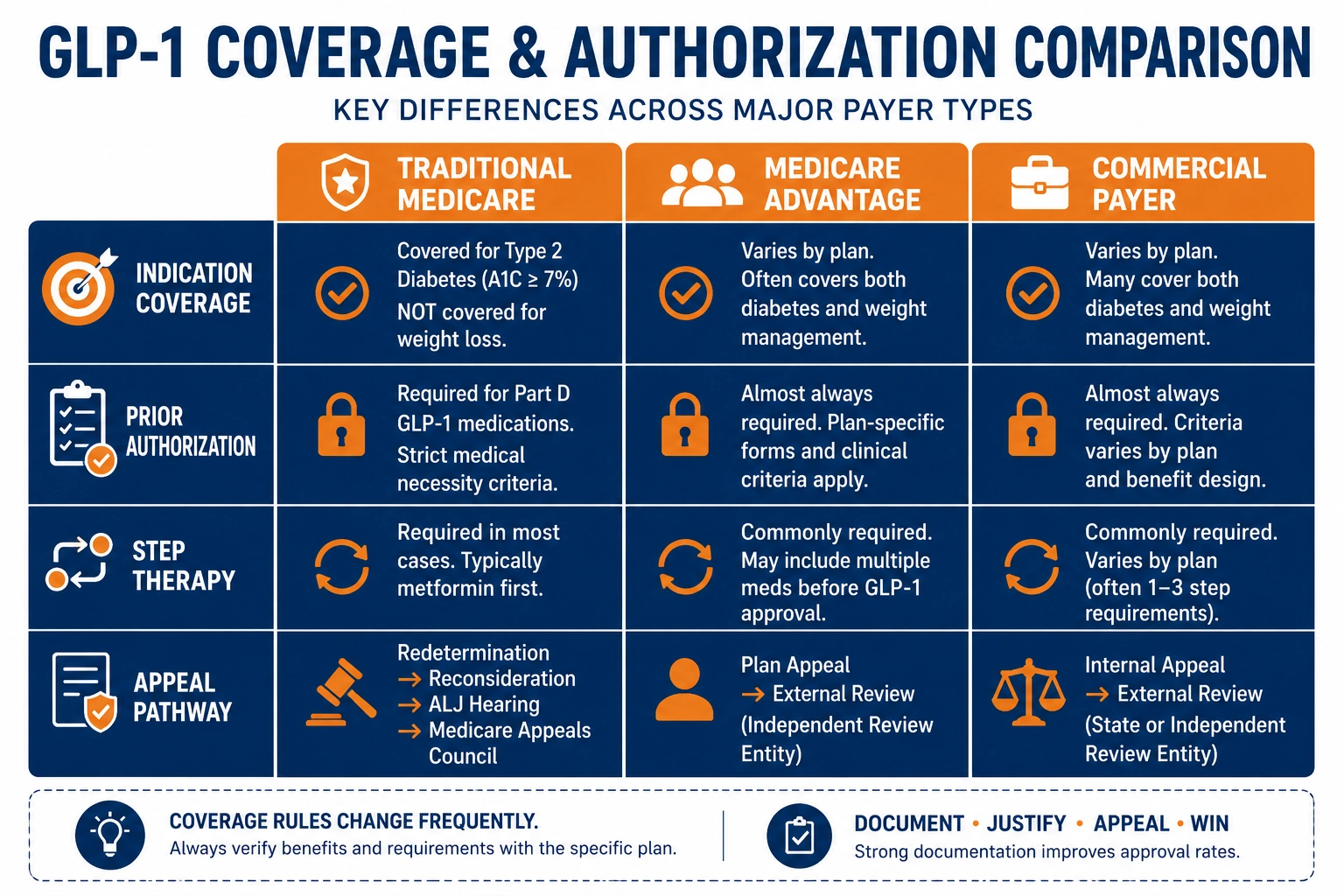
Traditional Medicare covers GLP-1 medications under Part D when prescribed for type 2 diabetes within FDA-approved labeling. Coverage for obesity-only indications remains restricted under traditional Medicare — a gap that continues to affect practices treating patients who do not carry a concurrent diabetes or cardiovascular diagnosis. Some improvement has occurred under CMS pilot programs and expanded cardiovascular indication coverage, but no permanent universal CMS GLP-1 coverage 2026 policy for weight loss has been codified. Select Medicare Advantage plans have started offering expanded GLP-1 formulary access for obesity indications, though coverage varies considerably by plan.
How Commercial Payers Differ From Medicare on GLP-1 Formulary Access
| Coverage Factor | Traditional Medicare | Medicare Advantage | Commercial Payer |
|---|---|---|---|
| Diabetes Indication | Part D (formulary-dependent) | Plan-specific formulary | Tier 3–4, PA required |
| Obesity Indication | Generally excluded | Select plans only | PA + step therapy required |
| Cardiovascular Risk | Expanding under Part D | Varies by plan | PA required, indication-specific |
| Prior Auth Required | Varies by plan | Yes — most plans | Yes — virtually universal |
| Step Therapy Required | No | Sometimes | Yes — most commercial plans |
| Appeals Pathway | Formal CMS process | Plan-level + CMS | Internal + external review |
Medicaid GLP-1 Coverage Variation by State
Medicaid coverage for GLP-1 medications varies widely by state. Some states have added GLP-1 agonists to their preferred drug lists for diabetes management. Others maintain strict commercial payer GLP-1 formulary restrictions, with narrow prior auth criteria and no obesity indication coverage at all. Your Medical Coding Services team must be equipped to manage state-specific Medicaid GLP-1 billing rules — they are not uniform, and treating them as a single national standard produces systematic, avoidable denials.
Documentation Requirements for GLP-1 Claims
What Must Be in the Clinical Note to Support GLP-1 Medical Necessity
Your clinical documentation must tell a complete medical story that justifies the GLP-1 prescription independently — meaning a reviewer with no other context should be able to read the note and understand exactly why this patient qualifies. At minimum, the medical necessity documentation for GLP-1 must include:
- Current BMI and weight trend over time
- HbA1c level with the date of measurement (for diabetes indications)
- Documented history of prior medications tried, with durations and outcomes
- Relevant comorbidities: hypertension, hyperlipidemia, ASCVD, sleep apnea
- An explicit medical necessity statement for GLP-1 therapy
- Treatment goals and a monitoring plan
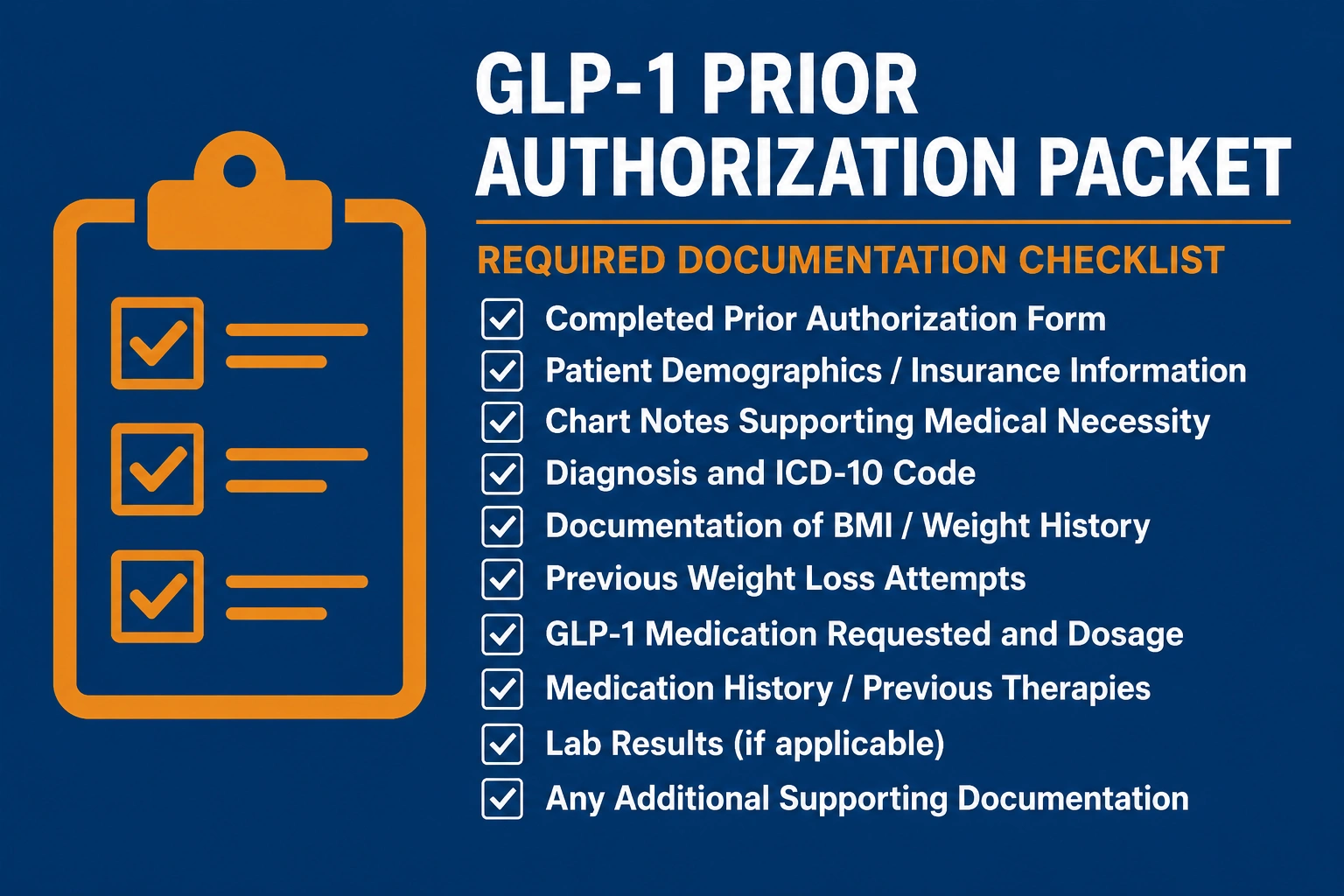
Prior Authorization Packets — What Payers Require in 2026
A complete prior auth packet for GLP-1 drugs typically includes the payer’s specific PA form, the supporting clinical note, recent lab results (HbA1c, lipid panel, BMI at current visit), a documented list of prior medications with trial durations and outcomes, and the prescribing physician’s attestation of medical necessity. Incomplete packets are returned or denied — and every day of delay is another day your patient cannot access the medication and another day your reimbursement sits in limbo.
Avoiding Common Documentation Errors That Trigger Audits and Clawbacks
Retrospective audits of GLP-1 claims are increasing as payer spend on these medications rises sharply. The following documentation errors are the most common triggers for post-payment audit findings and clawback demands:
- Copy-paste clinical notes without individualized documentation for each visit
- Failure to update BMI or lab values at GLP-1 follow-up appointments
- No documentation of patient response to therapy or dose adjustments over time
- Missing or incomplete step therapy records in the patient chart
Strategies Every Practice Should Implement Right Now
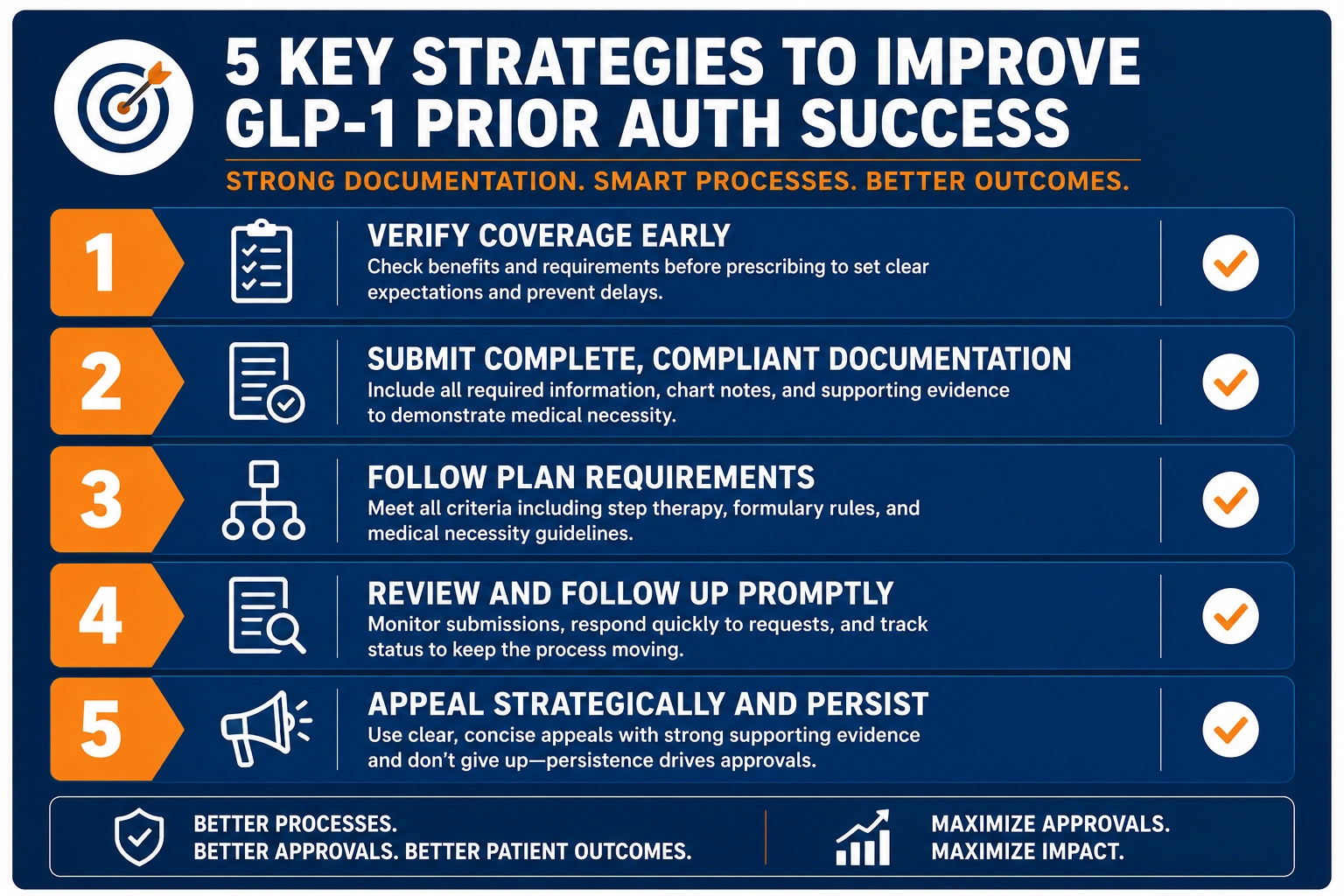
Verify GLP-1 Coverage and Prior Auth Requirements Before Prescribing
Make eligibility and formulary verification a standard step in the workflow before the prescription is written — not after the claim bounces. Knowing a payer’s GLP-1 formulary tier and prior auth criteria upfront eliminates reactive denials downstream and reduces the time-to-reimbursement significantly.
Use the Correct Diagnosis Code Combination for Each Payer
Maintain a payer-specific ICD-10 crosswalk for GLP-1 claims. Not every payer accepts the same code combination for the same drug and indication — and the divergence between diagnosis codes for GLP-1 prescribing across payers is wider than most practices realize. Document the primary diagnosis code along with all supporting secondary codes that reflect the patient’s complete clinical picture, and update the crosswalk whenever payers release new clinical criteria.
Build a Standardized Prior Authorization Workflow for GLP-1 Drugs
Create a repeatable, staff-managed workflow for initiating, tracking, and following up on GLP-1 prior authorizations. Assign clear ownership, set internal turnaround targets, and flag all pending authorizations before prescription fills are scheduled. A workflow that relies on memory or informal communication will produce gaps that cost you revenue.
Train Your Billing Staff on Payer-Specific GLP-1 Formulary and Step Therapy Rules
GLP-1 insurance coverage rules are not static. Payers update formularies, revise step therapy requirements for GLP-1 payers, and modify prior auth criteria regularly — sometimes multiple times per year. Your billing staff needs current, payer-specific training on GLP-1 drug billing 2026 rules, or they need to be partnered with a billing team that tracks these changes as a core function.
Outsource GLP-1 and High-Cost Drug Billing to Specialists
For many practices, the volume and complexity of GLP-1 billing makes fully internal management inefficient and risky. Dedicated Medical Billing Services built around high-cost specialty drug reimbursement can increase your first-pass approval rates, reduce rework cost, and recover the revenue your current workflow is losing quietly every month.
How Outsourced GLP-1 Medical Billing Protects Your Revenue
Proactive Prior Auth Denial Prevention for GLP-1 Claims
A specialized billing partner does not wait for denials to land. Proactive coverage verification, pre-submission claim audits, and payer-specific documentation checklists stop denials before they happen — keeping your GLP-1 revenue flowing without the rework cycle that drains your internal team’s time and energy.
Faster, Fully Documented Appeals With Clinical Evidence
When denials do occur, speed and documentation quality determine whether appeals succeed. An experienced GLP-1 medical billing team knows exactly which clinical evidence each payer requires in an appeal, and builds and submits those packets faster and more completely than in-house staff juggling multiple competing billing priorities.
Can Small Practices Get Reimbursed for GLP-1 Prescriptions?
Small and independent practices can absolutely get reimbursed for GLP-1 prescriptions — but it requires the same documentation rigor, payer-specific coding knowledge, and prior authorization discipline as any larger group. The difference is capacity. For smaller teams, outsourcing GLP-1 and high-cost drug billing becomes a practical necessity rather than a luxury. A specialized revenue cycle partner levels the playing field by handling payer monitoring, denial management, and documentation auditing that most small internal teams cannot sustain alongside their day-to-day workload.
Payer-Specific GLP-1 Denial Tracking and Trend Reporting
Tracking denials by payer, diagnosis code, and denial reason reveals systematic workflow problems before they become revenue crises. Granular trend reporting turns denial data into actionable process improvements — the kind of intelligence that most in-house billing teams do not have the bandwidth or tooling to generate consistently.
How Utreatibill Helps Practices Maximize GLP-1 Reimbursement
At Utreatibill, our revenue cycle management team works with healthcare practices that need specialized expertise in high-cost, high-complexity drug billing. We combine current payer intelligence, clinical documentation support, and proactive denial management to protect your GLP-1 revenue from the first submission through final payment.
Our team tracks CMS GLP-1 coverage 2026 updates, commercial payer formulary changes, and state-level Medicaid GLP-1 rule shifts in real time — so your billing workflow does not fall behind when the rules change. We know what documentation triggers approval and what triggers audits. We know which payers have changed their step therapy requirements and which diagnosis code combinations are being challenged in 2026. That knowledge is what separates consistent reimbursement from a cycle of denials, rework, and written-off revenue.
Key Takeaways
- GLP-1 medical billing requires precise alignment of ICD-10 diagnosis codes, HCPCS or NDC codes, prior authorization documentation, and payer-specific clinical criteria.
- The most common denial causes are missing prior authorization, incorrect diagnosis codes, and incomplete step therapy documentation.
- Medicare Part D covers GLP-1 medications for type 2 diabetes; obesity-only indications remain largely excluded from traditional Medicare in 2026.
- Clinical documentation must support medical necessity at every visit — not just at initiation of therapy.
- Practices without a dedicated GLP-1 billing workflow are almost certainly losing significant reimbursement every month without knowing exactly how much.
- Ozempic billing and reimbursement — along with weight loss drug billing for Wegovy and Zepbound — requires ongoing payer monitoring and staff training to maintain consistent revenue.
- Understanding GLP-1 prior authorization requirements by payer in 2026 and building a workflow around them is the single most impactful step most practices can take right now.
Final Thoughts
GLP-1 medications are transforming how clinicians approach type 2 diabetes, obesity, and cardiovascular disease management. But the complexity of GLP-1 medical billing is keeping too many practices from capturing the revenue they have legitimately earned. Whether the challenge is prior authorization for GLP-1, selecting the correct code combination, or navigating payer-specific formulary restrictions, the solution starts with a billing strategy built specifically for this class of medications.
The practices getting GLP-1 reimbursement right in 2026 are not just recovering denied claims. They are preventing denials in the first place — and they are doing it by partnering with revenue cycle specialists who understand GLP-1 drug billing 2026 inside and out.