
Pediatric CPT Codes 2026: Age-Banded Preventive Visit Guide
Getting pediatric CPT codes right is the difference between a clean claim and a denial that eats into your revenue cycle for weeks. In 2026, payers are auditing age-band selection, vaccine administration pairing, and modifier 25 usage more closely than ever — and a single mismatched code on a well-child visit can cost your practice the full reimbursement. This guide walks your billing team through the current pediatric CPT codes, the ICD-10 pairings payers expect, and the documentation that keeps preventive claims out of the denial pile.
What Are Pediatric CPT Codes in 2026?
Pediatric CPT codes are the procedure codes used to bill preventive checkups, sick visits, vaccine administration, and other pediatric procedure codes for patients from birth through young adulthood. They include age-banded preventive medicine CPT codes (99381–99397) — also called pediatric well-child visit codes 2026 — E/M sick-visit codes, and vaccine product and administration codes, each paired with a supporting ICD-10 diagnosis.
Pediatric CPT codes are the billing codes pediatricians use for well-child exams, sick visits, and immunizations. They include age-banded preventive medicine CPT codes (99381–99397), E/M codes for problem visits, and vaccine administration codes like 90460 and 90461. Correct code selection by patient age and visit type determines whether a claim is paid or denied.
Why Age-Banded Coding Accuracy Is a Revenue Priority for Every Pediatric Practice
Pediatric preventive medicine CPT codes are structured by age band on purpose — each bracket reflects a different scope of exam, screening, and counseling under the Bright Futures guidelines. When your team selects the wrong band, the claim doesn’t just get reduced; it gets denied outright, because payers edit preventive codes against the patient’s date of birth automatically.
What Changed in Pediatric Billing After Recent CMS and Payer Policy Shifts
The biggest 2026 change for pediatric immunization billing codes 2026 is the addition of three new time-based counseling codes: 90482, 90483, and 90484, for immunization counseling visits where no vaccine is actually given that day. Medicare won’t reimburse them, but check each commercial and Medicaid payer’s policy before billing, since coverage varies.
CMS and CPT Updates and What’s Permanent in 2026
CMS pediatric billing 2026 guidance keeps the core preventive code set (99381–99397) and vaccine administration logic unchanged. What’s new sits at the margins — counseling-only codes, refreshed telehealth guardrails, and continued emphasis on clean claim submission as payers lean harder on automated, AI-driven claim edits.
Why Many Practices Are Still Leaving Preventive Visit Reimbursement on the Table
Many practices still bill a single E/M code for a visit that included a preventive exam, a problem-focused evaluation, and vaccines — collapsing three billable services into one and writing off the difference without realizing it.
The Hidden Revenue Risk of Incorrect Age-Band Selection
A toddler coded under the wrong band, or a 6-year-old billed as “late childhood” instead of “early childhood,” triggers an instant payer edit. Multiply that across your daily schedule and the lost revenue compounds fast.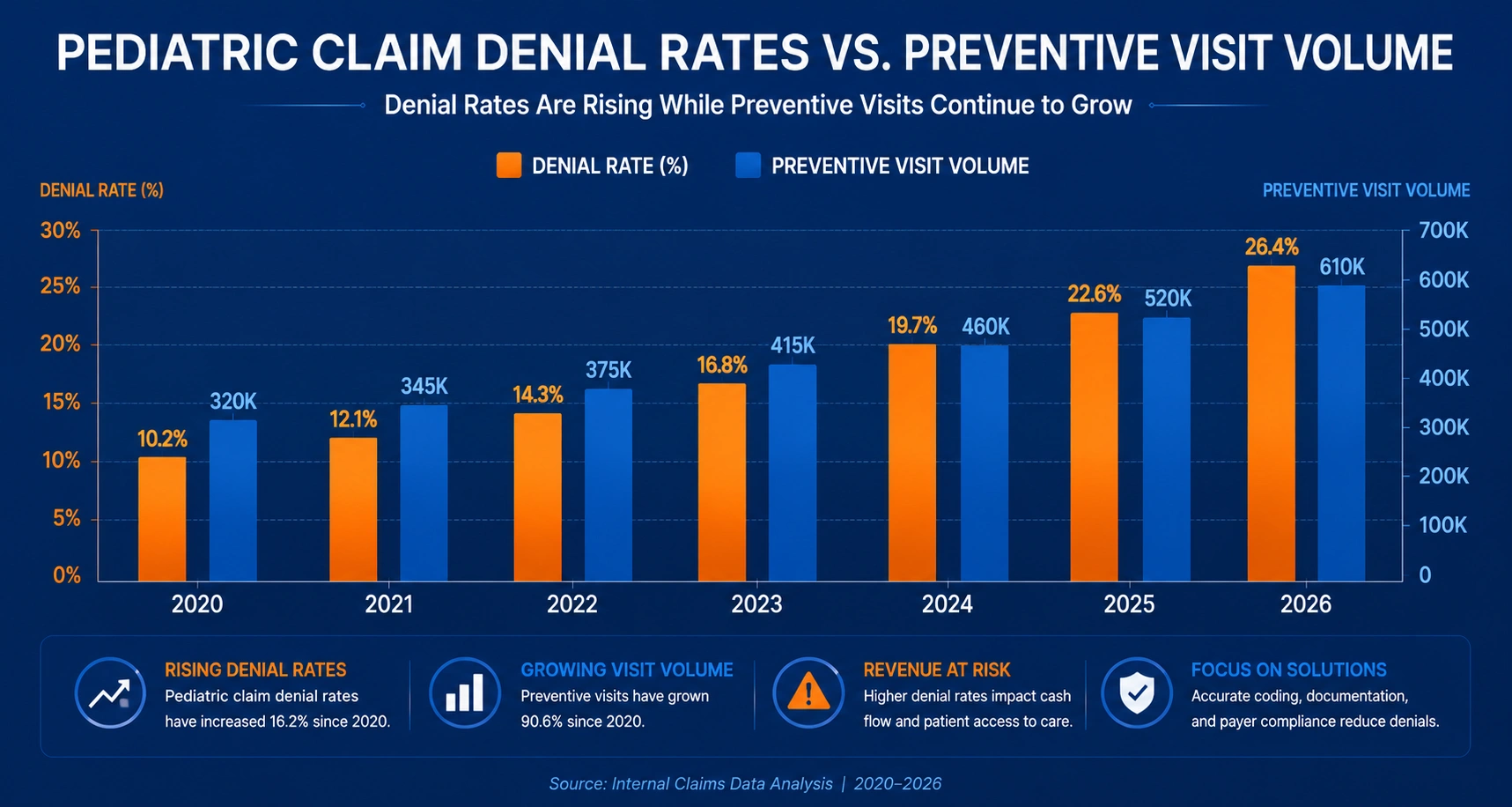
The Biggest Causes of Pediatric Billing Denials in 2026
Most pediatric claim denials trace back to a handful of repeatable mistakes. Here’s where your billing team should focus first.
Age-Band Mismatches Between Patient Age and CPT Code
Age-band selection errors in pediatric coding happen most often around birthday transitions — a patient turns 5 between scheduling and the visit date, and the front desk doesn’t update the code.
Wrong ICD-10 Diagnosis Codes — Well Visit vs. Sick Visit
Pairing a sick-visit ICD-10 code with a preventive CPT code (or vice versa) is an automatic mismatch in most payer systems.
Medicaid/EPSDT Outpatient Billing Confusion
Medicaid EPSDT outpatient pediatric billing rules vary by state and by managed care organization, so a workflow built for one state’s Medicaid program can generate denials when applied to another.
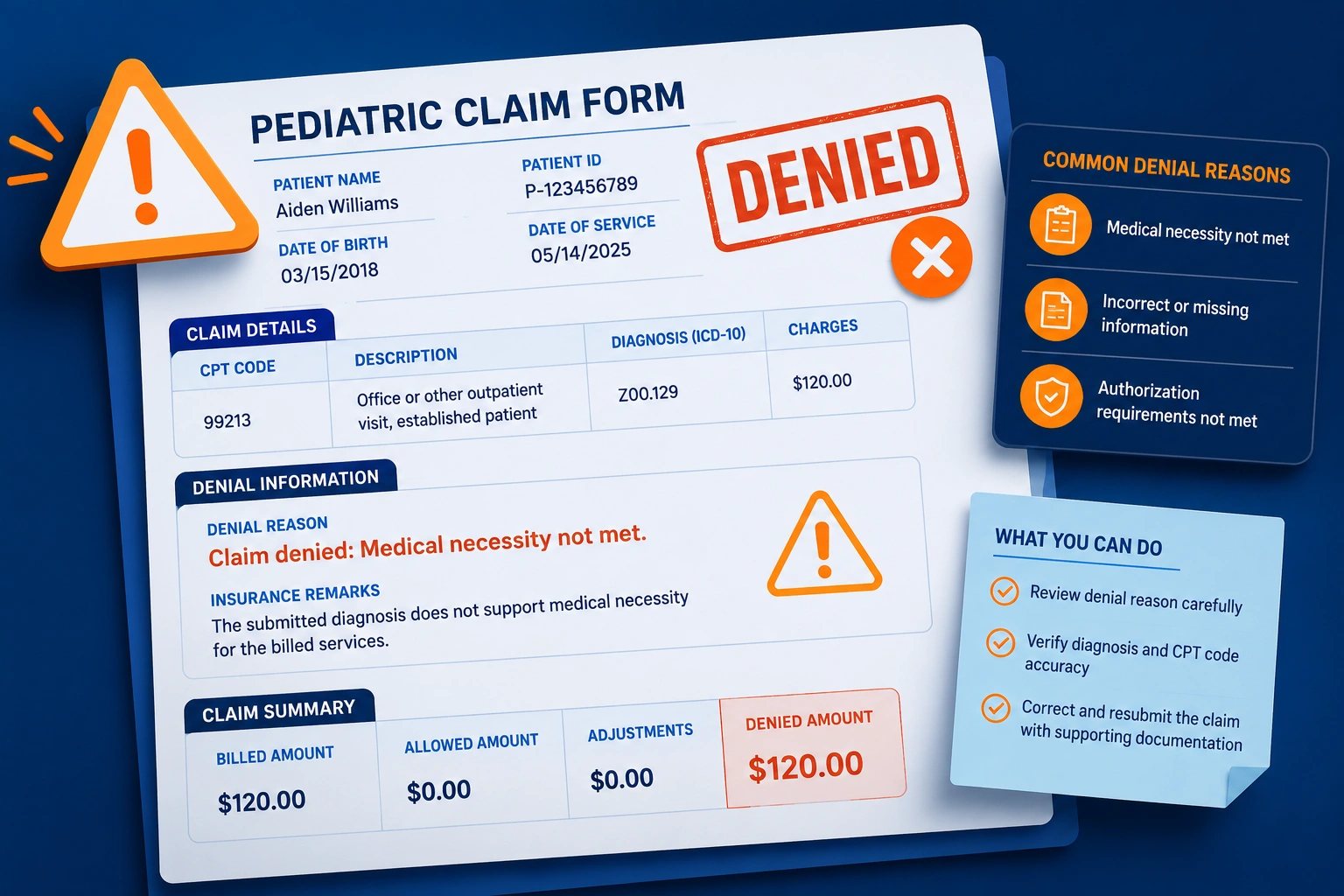
Documentation Gaps That Trigger Automatic Denials
If the clinical note doesn’t separately document the preventive exam and the problem visit, payers have no basis to pay both services.
Confusing Preventive Codes With E/M Sick-Visit Codes
Preventive visit codes cover a comprehensive, age-appropriate exam. E/M codes for sick visits with modifier 25 cover a separately identifiable problem addressed on the same day — billing one in place of the other shortchanges your practice.
Modifier 25 Errors on Same-Day Visits
Forgetting modifier 25 on the E/M code — or appending it without documentation that proves the problem visit was distinct from the preventive exam — is one of the most common, and most fixable, pediatric denial reasons.
The Complete Pediatric CPT Codes 2026 Billing Guide
This section is your quick-reference for the pediatric well-child visit codes 2026 and pediatric preventive medicine CPT codes your team uses every day.
Age-Banded Preventive Visit Codes — 99381–99397
New patient vs. established patient preventive codes 99381–99397 are split by patient status and age:
| Age Band | New Patient | Established Patient |
|---|---|---|
| Infant (under 1 year) | 99381 | 99391 |
| Early childhood (1–4 years) | 99382 | 99392 |
| Late childhood (5–11 years) | 99383 | 99393 |
| Adolescent (12–17 years) | 99384 | 99394 |
| Young adult (18–20, EPSDT-eligible) | 99385 | 99395 |
Use the established-patient column for any patient seen at your practice within the past three years; new-patient codes apply only when no professional service has been provided in that window.
ICD-10 Codes That Support Medical Necessity for Well-Child Visits
ICD-10 codes for well-child visits (Z00.110, Z00.121, Z00.129) are the diagnosis pairings payers expect on a preventive claim. Z00.110 applies to a newborn health exam at 8 days old or younger. Z00.129 is the standard code for a routine child health exam with no abnormal findings, while Z00.121 is used when the exam identifies an abnormal finding — which can also support billing a separate problem-focused E/M with modifier 25.
Vaccine Product and Administration Codes (90460, 90461, and Add-Ons)
Vaccine administration codes 90460 vs. 90461 are reported per component, not per shot, and they’re the backbone of accurate pediatric immunization billing codes 2026. Bill 90460 for the first component of each vaccine product (when a physician or qualified health professional provides face-to-face counseling to a patient 18 or younger), then 90461 — a pediatric modifier-style add-on code — for every additional component in that same product. A three-component DTaP, for example, is one unit of 90460 plus two units of 90461. Without documented counseling, use 90471–90474 instead.
Telehealth Pediatric CPT Codes and Modifier Requirements
Telehealth pediatric billing codes generally follow standard E/M codes reported with place-of-service 02 or 10 and modifier 95 for synchronous audio-video visits, though coverage for preventive exams via telehealth still varies widely by state Medicaid program and commercial payer — many require an in-person component for the physical exam elements of a well-child visit.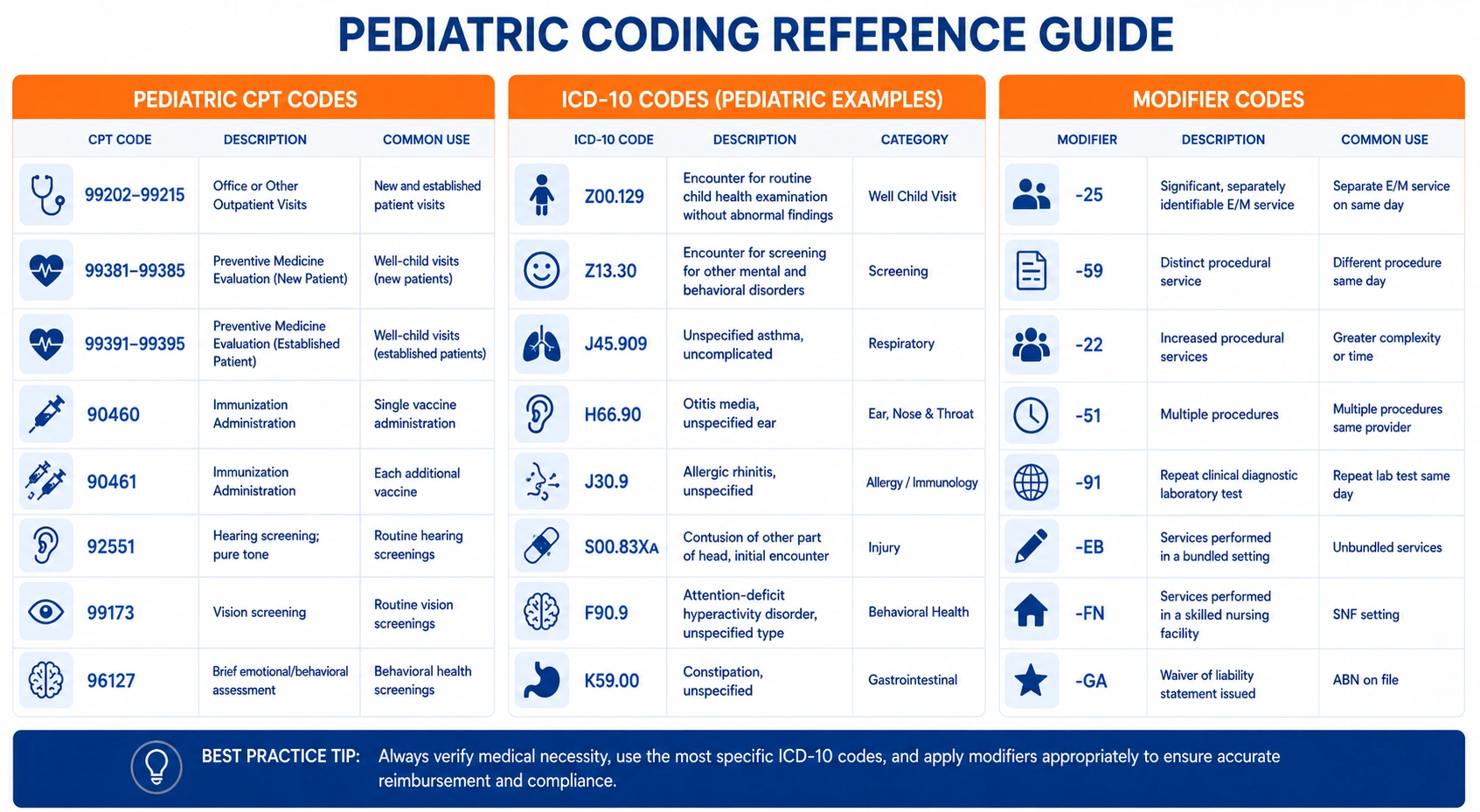
How Much Revenue Is Your Practice Losing to Pediatric Billing Errors?
These scenarios show how small coding slips translate into real dollars across a busy pediatric schedule.
Example 1 — Wrong Age Band Leads to a Denied Preventive Claim
A 5-year-old is billed as 99392 (early childhood) instead of 99393 (late childhood) because the front desk didn’t catch a recent birthday. The payer’s system flags the age mismatch and denies the entire preventive claim — not just the difference in value.
Example 2 — Missing Modifier 25 on a Same-Day Sick Visit
A child comes in for a well-child visit and the parent mentions a persistent ear infection. The provider documents and treats both, but the billing team submits only the preventive code. The separately billable E/M with modifier 25 — and its reimbursement — never gets captured.
Example 3 — Vaccine Administration Stacking Errors
A patient receives three vaccines with a total of seven components. The biller submits three units of 90460 and stops there, missing four units of 90461. That’s four underbilled administration units on a single visit, repeated across every immunization-heavy day on the schedule.
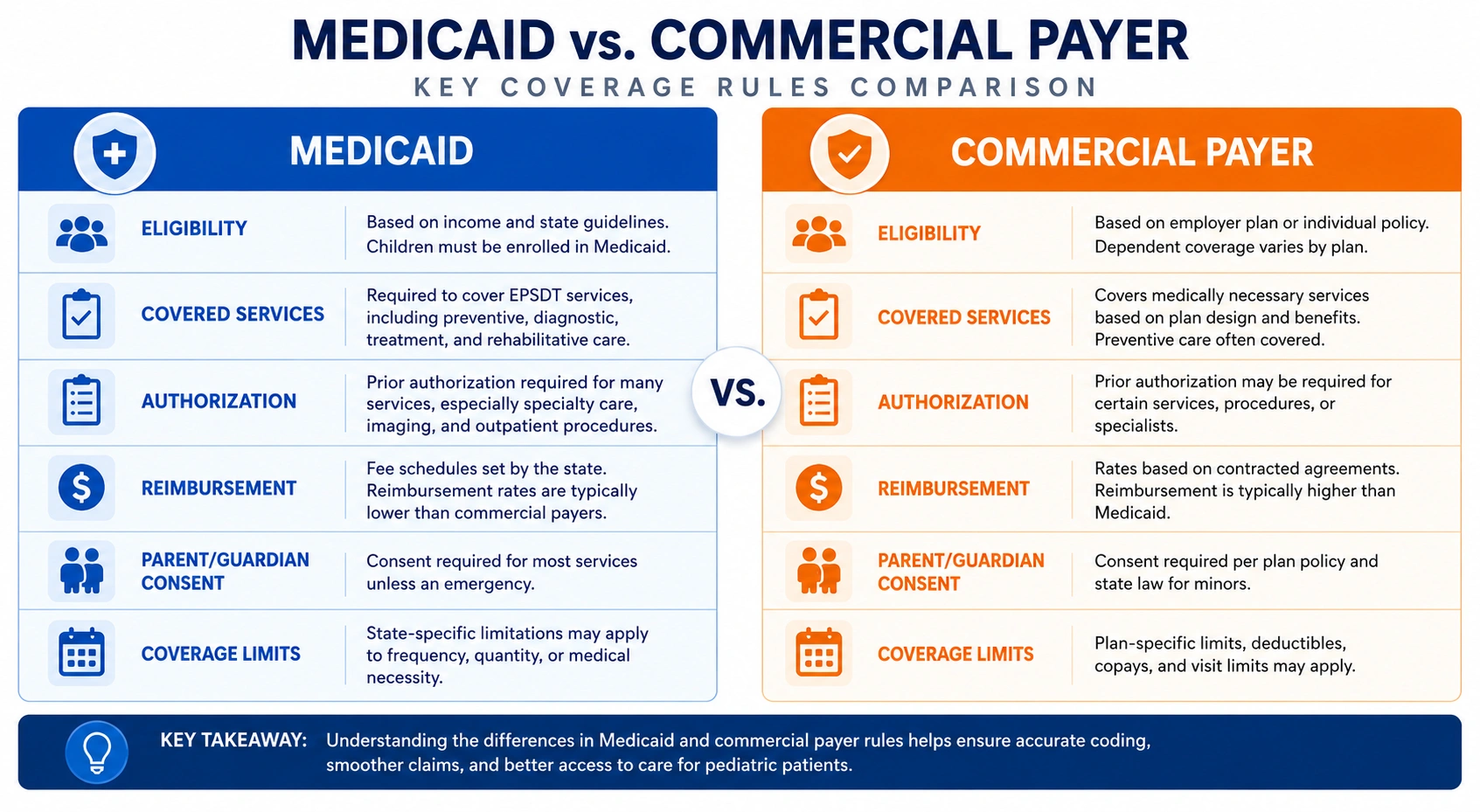
Medicaid vs. Commercial Payer Pediatric Rules: A 2026 Comparison
Your billing team needs separate playbooks for Medicaid and commercial claims — the rules genuinely differ.
What Medicaid/EPSDT Covers for Pediatric Preventive Care in 2026
Medicaid EPSDT outpatient pediatric billing is a mandatory benefit covering periodic comprehensive health and developmental assessments for enrollees under 21, with required screenings tied to the state’s periodicity schedule.
How Commercial Payers Differ From Medicaid on Pediatric Coverage
Commercial payer prior authorization for pediatric services is more likely to apply to developmental and behavioral health screenings than to routine preventive exams, while Medicaid documentation standards are often stricter overall.
State-by-State Medicaid Pediatric Coverage Variation
Each state Medicaid program — and each managed care organization within it — sets its own prior authorization list, timely filing window, and vaccine billing rules, so a workflow that works in one state can generate denials in another.
| Factor | Medicaid/EPSDT | Commercial Payers |
|---|---|---|
| Eligibility for preventive coverage | Mandatory benefit, under age 21 | Varies by plan; typically follows ACA preventive mandate |
| Prior authorization | Often required for behavioral/developmental screens | More likely for specialty referrals, less for routine well visits |
| Documentation standard | Frequently stricter, state-specific | Payer-specific, generally less prescriptive |
| Timely filing | Commonly 90–365 days, varies by state | Commonly 90–180 days |
| Reimbursement rate | Generally lower than commercial rates | Generally higher base reimbursement |
Documentation Requirements for Pediatric Claims
Clean documentation is what survives an audit — and what gets your appeals approved the first time.
What Must Be in the Clinical Note to Support Medical Necessity
The note needs a clearly separated preventive component (age-appropriate history, exam, screening, anticipatory guidance) and, if applicable, a distinct problem-focused assessment and plan to support modifier 25.
Prior Authorization Packets — What Payers Require in 2026
Pediatric prior authorization requirements by payer 2026 generally call for the clinical note, relevant screening tool scores, and a clear statement of medical necessity tied to the requested service.
Avoiding Common Documentation Errors That Trigger Audits and Clawbacks
Vague templates that mark “counseling provided” by default — without recording what was actually discussed — are a frequent audit trigger for vaccine administration codes specifically.
Strategies Every Pediatric Practice Should Implement Right Now
These are the habits that move denial rates down fastest.
Verify Coverage and Prior Auth Requirements Before Scheduling
Confirm eligibility, plan-specific preventive coverage, and any prior auth needs before the visit, not after the claim is denied.
Use the Correct Age-Band and Diagnosis Code Combination for Each Payer
Build age-banded E/M and preventive code templates into your EHR so the system pre-populates the right code range for each patient’s birthdate.
Build a Standardized Workflow for Well-Visit/Sick-Visit Same-Day Billing
Yes — small pediatric practices can get reimbursed for same-day sick and well visits, but only with a documented, repeatable process for separating the two services and applying modifier 25 consistently.
Train Your Billing Staff on Payer-Specific Pediatric Rules
Your billing team should maintain a living cheat sheet of each major payer’s pediatric-specific rules, updated whenever a payer policy changes.
Outsource Pediatric Billing to Specialists
If your in-house team is stretched across every specialty your practice touches, pediatric-specific billing knowledge is often the first thing to slip — which is where a dedicated partner closes the gap. Our Medical Coding Services team builds payer-specific pediatric coding workflows so age-band and modifier errors get caught before submission, not after denial.
How Outsourced Pediatric Billing Protects Your Revenue
Proactive Denial Prevention for Pediatric Claims
Catching age-band mismatches, missing modifiers, and vaccine stacking errors before submission is far cheaper than reworking a denial after the fact.
Faster, Fully Documented Appeals With Clinical Evidence
When a denial does happen, a documented appeal built from the clinical note and payer policy resolves faster than a generic resubmission.
Payer-Specific Pediatric Denial Tracking and Trend Reporting
Tracking denials by payer and reason surfaces patterns — like one Medicaid MCO consistently rejecting a specific vaccine code — before they become a six-figure problem.

How UtreatiBill Helps Pediatric Practices Maximize Reimbursement
At UtreatiBill, our revenue cycle management team builds pediatric billing workflows around the realities of your schedule — same-day sick and well visits, immunization-heavy days, and multi-payer Medicaid mixes. We pair pediatric medical billing services with payer-specific denial tracking so age-band errors, modifier 25 gaps, and vaccine stacking mistakes get caught before they cost your practice a dollar.
The Financial Cost of Pediatric Billing Errors in 2026
The numbers behind pediatric billing errors are sobering for any practice running on thin margins.
- Rising visit volume meets rising denial risk: As preventive visit volume grows year over year, payers have responded by tightening automated claim edits — meaning more volume doesn’t automatically mean more clean reimbursement.
- Cost to rework a denied claim: Industry data from HFMA and MGMA puts the average cost to rework a single denied claim between $25 and $118, a cost that compounds quickly across a high-volume pediatric schedule.
- Denial rate benchmarks: MGMA reports that best-performing practices keep denial rates under 4–5%, while many specialty practices run at 10% or higher without realizing it.
- Medicaid vs. commercial reimbursement gaps: Medicaid fee-for-service physician payments typically run well below commercial reimbursement for the same preventive service, widening the revenue gap for practices with a heavy Medicaid/EPSDT patient mix.
- The volume-to-reimbursement gap: A large share of denied claims are never reworked at all, meaning a meaningful slice of delivered, billable pediatric care is simply written off rather than collected.
Key Takeaways
- Pediatric CPT codes are organized by age band, and getting the band wrong is the single most common cause of preventive claim denials.
- Vaccine administration codes 90460/90461 are billed per component, not per injection — undercounting components quietly erodes revenue.
- Modifier 25 is what makes same-day sick and well visits billable as two services instead of one.
- Medicaid/EPSDT and commercial payers have genuinely different documentation, prior auth, and reimbursement rules — one workflow doesn’t fit both.
- Clean, separated clinical documentation is your best defense against both denials and audits.
Final Thoughts
Pediatric CPT codes will keep evolving — new counseling codes, shifting telehealth rules, tighter payer edits — but the fundamentals stay the same: the right age band, the right diagnosis pairing, and documentation that backs up every code you bill. If your billing team is stretched thin trying to track all of it across every payer, that’s exactly the gap our revenue cycle management team at UtreatiBill is built to close. Reach out and let’s look at where your pediatric claims are losing revenue.

