CMS Prior Authorization Rule 2026: What Every Medical Practice Must Do Now to Avoid Revenue Loss
The prior authorization rule 2026 is not on the horizon — it is already here, and it is already costing unprepared practices real revenue. As of January 1, 2026, the Centers for Medicare & Medicaid Services began enforcing the compliance deadlines embedded in CMS-0057-F, the Interoperability and Prior Authorization Final Rule. These changes directly reshape how your practice submits, tracks, and appeals prior authorizations across Medicare Advantage, Medicaid managed care, and CHIP plans.
If your billing team has not updated its workflows to match the new requirements, you are already behind. The practices we see struggling most right now are the ones that assumed the transition would take care of itself. It has not. At UtreatiBill, our Revenue Cycle Management Services team works with physician groups and specialty practices every week, and the gap between compliant and non-compliant workflows is already showing up in denial rates and revenue loss.
This guide breaks down exactly what changed, which payers and practices are affected, what gold carding really means in 2026, and what your practice needs to do right now to protect revenue.
What Is the CMS Prior Authorization Rule 2026?
Quick Answer The CMS Prior Authorization Rule 2026, finalized under CMS-0057-F (the Interoperability and Prior Authorization Final Rule), requires Medicare Advantage plans, Medicaid, and CHIP managed care organizations to implement electronic prior authorization (ePA) systems, issue urgent decisions within 72 hours, issue standard decisions within 7 calendar days, and disclose specific written reasons for every prior authorization denial.
The rule’s compliance deadlines took effect January 1, 2026. At its core, CMS-0057-F mandates the adoption of HL7 FHIR-based APIs to accelerate electronic prior authorization exchange between payers and providers — replacing slow, manual fax-and-phone workflows with structured, trackable digital processes.
At a glance, the rule covers:
- Affected payers: Medicare Advantage organizations, Medicaid managed care plans, CHIP programs, and federally facilitated marketplace QHP issuers
- Affected practices: Any provider billing those payers, including primary care, specialty, surgical, and behavioral health
- Decision timelines: 72 hours for urgent requests; 7 calendar days for standard requests
- Denial requirements: Payers must provide specific, clinically relevant written reasons — not generic codes
- Public transparency: Payers must report prior authorization metrics publicly beginning in 2026
One important boundary: commercial fully-insured and self-funded employer plans remain largely outside the scope of CMS-0057-F. That distinction matters if your practice has a mixed payer population.
Why the Prior Authorization Rule 2026 Is Changing Everything for Practices
What Exactly Changed on January 1, 2026
Before 2026, prior authorization turnaround timelines were largely payer-governed. Some Medicare Advantage plans routinely took 14 to 21 days on non-urgent requests. Under CMS prior authorization 2026 requirements, that is no longer permitted for covered payers.
Your billing team needs to understand the practical shift:
- Payers must implement Prior Authorization Support (PAS) APIs using HL7 FHIR standards
- Urgent requests: decisions required within 72 hours
- Standard requests: decisions required within 7 calendar days
- All denials: payers must provide written, clinically specific reasons
- Payer denial data: now publicly reportable — your practice can benchmark against it
That last point opens a real strategic opportunity. Published payer-level denial data means you can identify which plans are denying most aggressively and adjust your submission strategy accordingly. But only if someone on your team is monitoring it.
The New 7-Day Decision Window and Mandatory Denial Reasons
The 7-day standard decision window seems reasonable on paper. In practice, it changes how your staff must approach prior auth follow-up.
Old workflow: Submit, wait, call to check status around day 10 to 14. New workflow: If no decision by day 7, something is wrong — escalate immediately.
The mandatory denial reason requirement shifts the appeal dynamic significantly. When a payer must give you a specific clinical reason for every denial, you have the documentation you need to mount a stronger, targeted appeal. That is a meaningful advantage — if your team knows how to use it.
Why Many Practices Still Haven’t Updated Their Workflows
Despite the January 2026 enforcement date, a large number of practices are still running outdated prior authorization processes. Common reasons include:
- Assumed payers would proactively notify them of process changes
- EHR vendor has not yet completed ePA integration
- Billing staff is stretched too thin to restructure workflows mid-cycle
- Uncertainty about which payers fall inside versus outside CMS-0057-F scope
None of these reasons reduce your exposure. Payers covered under the rule are now operating under new standards, and they are not extending grace periods because your workflows have not caught up.
The Hidden Revenue Risk of Missed Transition Deadlines
Missed transition deadlines do not just delay revenue — they result in:
- Denied claims that fall outside the new appeal window
- Compounding administrative rework costs on preventable denials
- Reduced provider productivity as billing staff manually chase payer status updates
The longer your practice waits, the more revenue accumulates in the “preventable loss” column.
The Financial Cost of Prior Authorization Delays and Denials in 2026
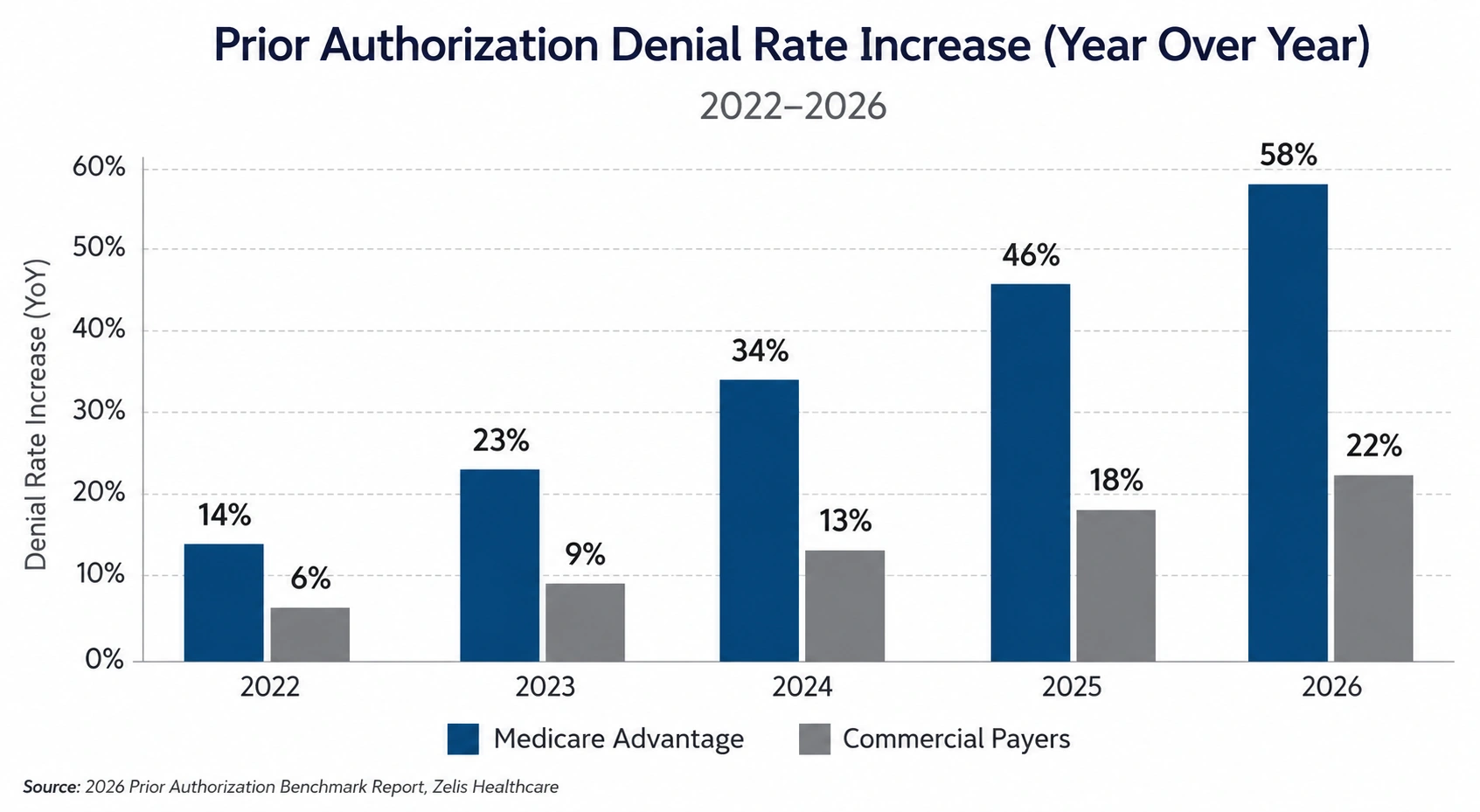
The numbers behind prior authorization burden in 2026 are significant — and they are trending in the wrong direction for practices that have not adapted.
- The American Medical Association’s 2024 Prior Authorization Physician Survey found that 94% of physicians report prior authorization delays patient care, and 89% say the administrative burden has increased over the past five years.
- MGMA research indicates that prior authorization denials cost the average medical practice between $68,000 and $85,000 per physician annually in administrative overhead and lost revenue.
- The average cost to rework a single denied prior authorization claim — including staff time, documentation, and resubmission — ranges from $43 to $196, according to HFMA benchmarking data.
- Medicare Advantage prior auth denials are statistically more likely to be overturned on appeal than fee-for-service denials — yet most practices never appeal. That is a direct revenue transfer from your practice to the payer.
- Gold carding laws have passed in more than 20 states, but enforcement gaps mean many eligible physicians continue submitting full prior auths for procedures they should be exempt from.
The Biggest Drivers Behind Rising Prior Authorization Denials in 2026
Understanding why denials happen is the foundation of proactive denial prevention. Here are the six most common drivers we see across our client practices right now.
Payer Automation and Algorithmic Denial Systems
Medicare Advantage plans and other managed care payers are increasingly using AI-driven systems to auto-flag and deny prior auth requests without clinical review. These algorithms make decisions based on code combinations, documentation completeness, and historical approval patterns.
The problem: algorithms do not understand clinical nuance. A missing modifier, an incomplete progress note, or a mismatched code combination can trigger an auto-denial in seconds. Your best defense against algorithmic denial systems is airtight documentation before the request ever leaves your office.
Medicare Advantage Plan Complexity
Medicare Advantage prior auth denials represent the most complex segment of prior authorization denial management right now. MA plans vary dramatically in their formularies, coverage policies, and required documentation — even among plans issued by the same parent organization.
A patient on Plan A and a patient on Plan B from the same insurer may require completely different prior auth supporting documentation for the identical procedure. Generic templates will not protect your revenue here.
Documentation Gaps That Trigger Auto-Denials
The most preventable cause of prior authorization denial remains incomplete or inconsistent documentation. The most frequent gaps your team should watch for:
- Missing clinical notes supporting medical necessity
- Outdated ICD-10 codes that do not match current payer policies
- Absent prior treatment failure documentation for step therapy requirements
- Unsigned or undated supporting clinical records
These gaps are correctable before submission. Every one of them that reaches the payer uncorrected represents unnecessary denial risk.

Inconsistent Gold Carding Enforcement Across States
Gold carding laws exist in more than 20 states — but payer enforcement is inconsistent. Physicians who believe they are gold-carded are sometimes still being required to submit full prior auths, leading to confusion, workflow errors, and denials that would never have happened under proper exemption.
New CPT Codes Outpacing Payer Rule Updates
CMS releases updated CPT codes annually. Payer prior authorization requirement databases do not always keep pace. This creates a gap — sometimes months long — where a new CPT code either has no payer policy or is evaluated under legacy criteria that do not match. Specialty practices in interventional cardiology, orthopedics, and oncology are especially exposed to this dynamic.
Staffing Gaps in Prior Auth Follow-Up
Prior authorization is not a submit-and-wait function. It requires active follow-up, documented payer responses, and timely escalation when decisions are delayed or unexpectedly denied. Under the new 7-day rule, a missing follow-up at day 8 may signal a payer compliance issue your practice should be documenting — not ignoring.
How Much Revenue Is Your Practice Losing to Prior Authorization Denials?
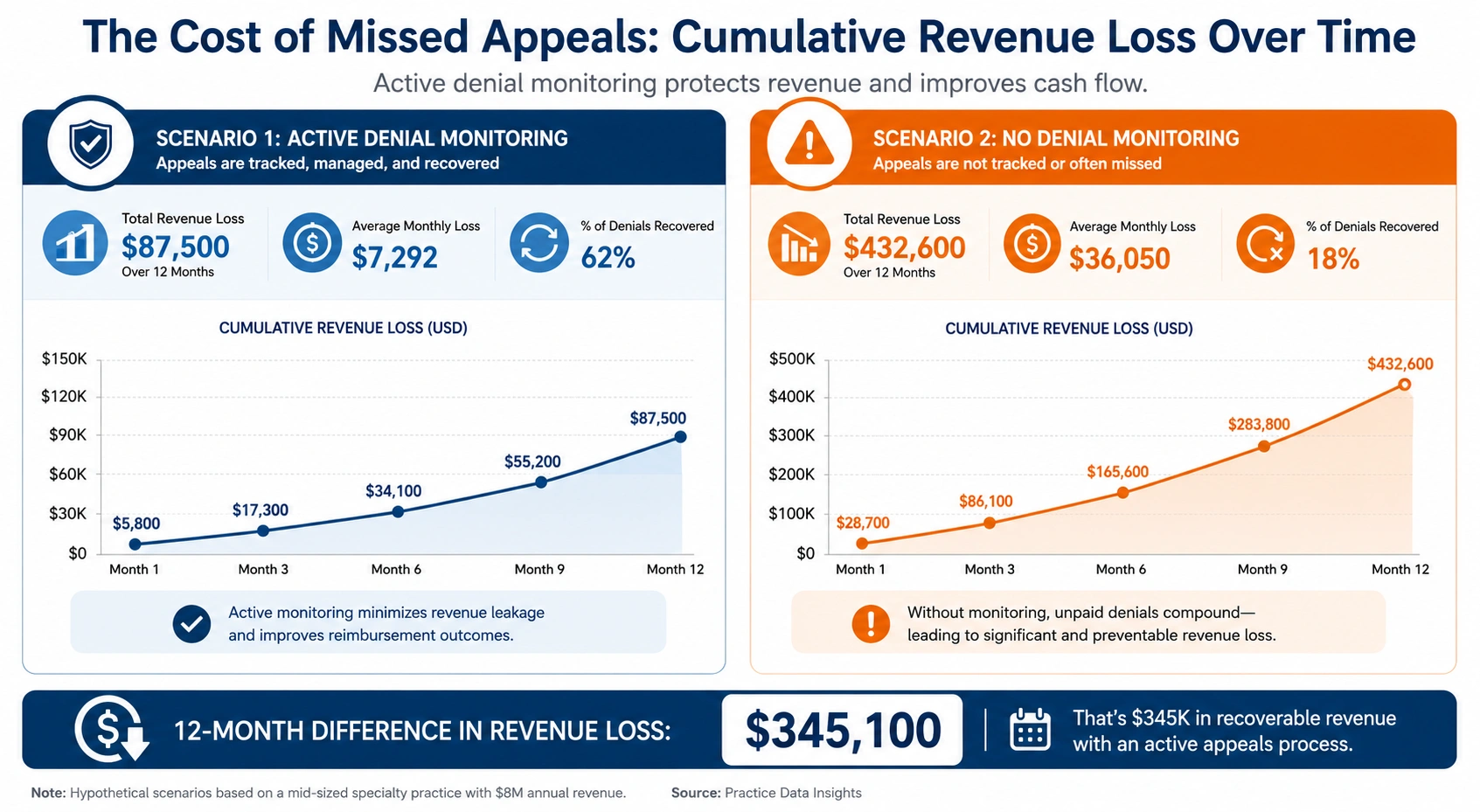
Example 1 — Missed Appeal Windows
A multi-provider orthopedic group submits prior auth for outpatient shoulder surgery. The payer denies it citing insufficient medical necessity documentation. The denial notice arrives on a Friday afternoon, sits unread until Tuesday, and by the time staff begins the appeal, the plan’s internal 30-day appeal window has closed.
Result: $4,800 in unrecoverable lost revenue on a single case. Multiply that across 15 to 20 similar cases per quarter, and this practice is losing $72,000 to $96,000 annually from missed appeal deadlines alone — all of it preventable.
Example 2 — High-Approval Physicians Still Getting Denied
A board-certified neurologist with a 96% historical prior auth approval rate for a specific diagnostic procedure begins receiving denials from a Medicare Advantage plan after a mid-year formulary update. Because no gold carding exemption is in place and the practice is not monitoring payer-specific denial patterns, six months pass before the trend is identified.
This is precisely the scenario that a monthly prior authorization audit prevents — catching payer behavior changes in 30 days instead of six months.
Example 3 — Specialty-Specific Denial Spikes
Oncology, behavioral health, and home health practices are seeing the steepest prior authorization denial increases under CMS prior authorization 2026 enforcement timelines. These specialties involve extended treatment courses with multiple separate authorization touchpoints — each one an independent denial risk.
For oncology specifically, a single chemotherapy regimen may require five to seven distinct prior authorizations over a treatment course. If two are denied and not appealed within window, the per-patient revenue impact is significant and compounds across a patient panel.
Gold Carding in 2026: What It Is and Why It’s Not Saving Practices Yet
Gold carding is a policy that exempts physicians with high prior authorization approval rates — typically 90% or above over a defined look-back period — from submitting prior auths for certain procedures or services. Instead of reviewing each request, the payer pre-approves, or “gold-cards,” those physicians.
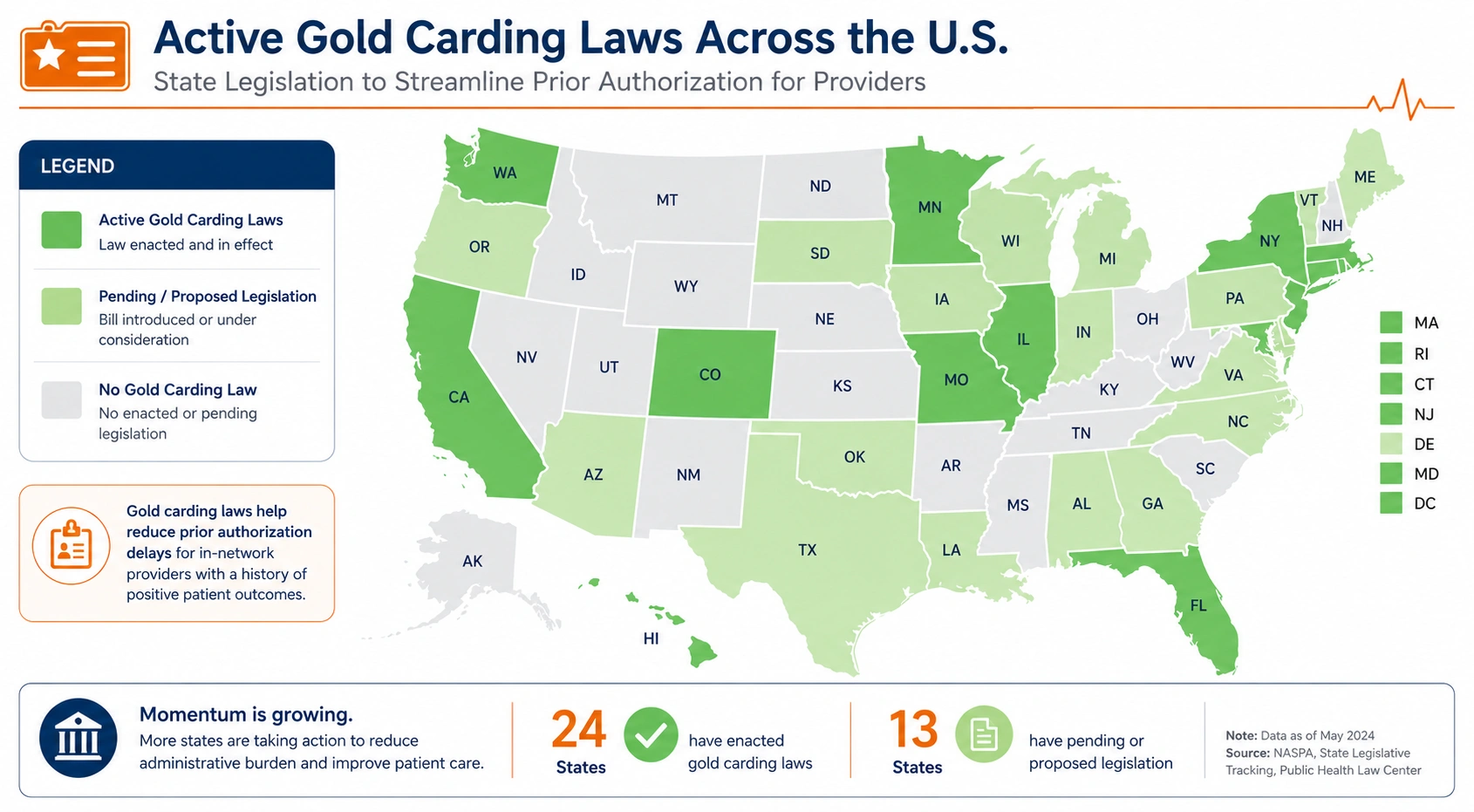
Which States Have Gold Carding Laws Right Now
As of 2026, gold carding laws have been enacted in Texas, West Virginia, Arkansas, Tennessee, Indiana, Michigan, and several additional states. Requirements vary: some mandate gold carding for any physician holding a 90% approval rate over six consecutive months; others set different thresholds or apply only to specific procedure categories.
The Gap Between Law and Payer Enforcement
Passing a law and enforcing it are two different things. Many payers in gold carding states are technically required to apply exemptions but have not implemented consistent enforcement systems. Practices whose physicians qualify for gold carding relief are often still submitting full prior auths — spending unnecessary staff time and delaying treatment without any compliance benefit.
Closing this gap requires active payer relationship management and documentation of each payer’s gold carding compliance status — not a one-time check, but an ongoing tracking function.
How to Check If Your Practice Qualifies
To assess gold carding eligibility across your payer mix, your billing team should:
- Pull prior authorization approval rates by physician and by payer for the past 12 months
- Identify which of your payers operate in states with active gold carding laws
- Compare physician-level approval rates against each state’s statutory threshold
- Submit formal written gold carding requests to qualifying payers
- Document payer responses and set quarterly eligibility review reminders
A structured medical billing audit is the most efficient way to complete this review systematically, rather than chasing it through manual tracking.
How to Identify Prior Authorization Denial Patterns in Your Practice
Key Warning Signs in Your Claims Data
The following patterns in your billing data indicate an emerging prior authorization denial problem that needs immediate attention:
- More than 5% of prior auth requests result in denial
- Appeal rate is below 30% of all denials received
- Denials from a single payer have increased in two or more consecutive months
- Denial reason codes are vague or repetitive (“not medically necessary” without clinical specifics)
- First-pass approval rate has declined since January 2026
Revenue Cycle Metrics to Monitor Monthly
| Metric | Benchmark Target | Red Flag Threshold |
|---|---|---|
| Prior auth denial rate | Below 5% | Above 8% |
| First-pass approval rate | Above 85% | Below 75% |
| Appeal overturn rate | Above 50% | Below 30% |
| Average prior auth turnaround | Under 7 days | Over 10 days |
| Gold carding compliance | 100% of eligible | Any unexplained gap |
| Claims rework cost per denial | Below $50 | Above $100 |
Tracking these metrics monthly creates an early-warning system that catches denial pattern shifts before they compound into significant revenue loss. If your billing team is not currently running this kind of revenue cycle automation reporting, now is the time to build it.
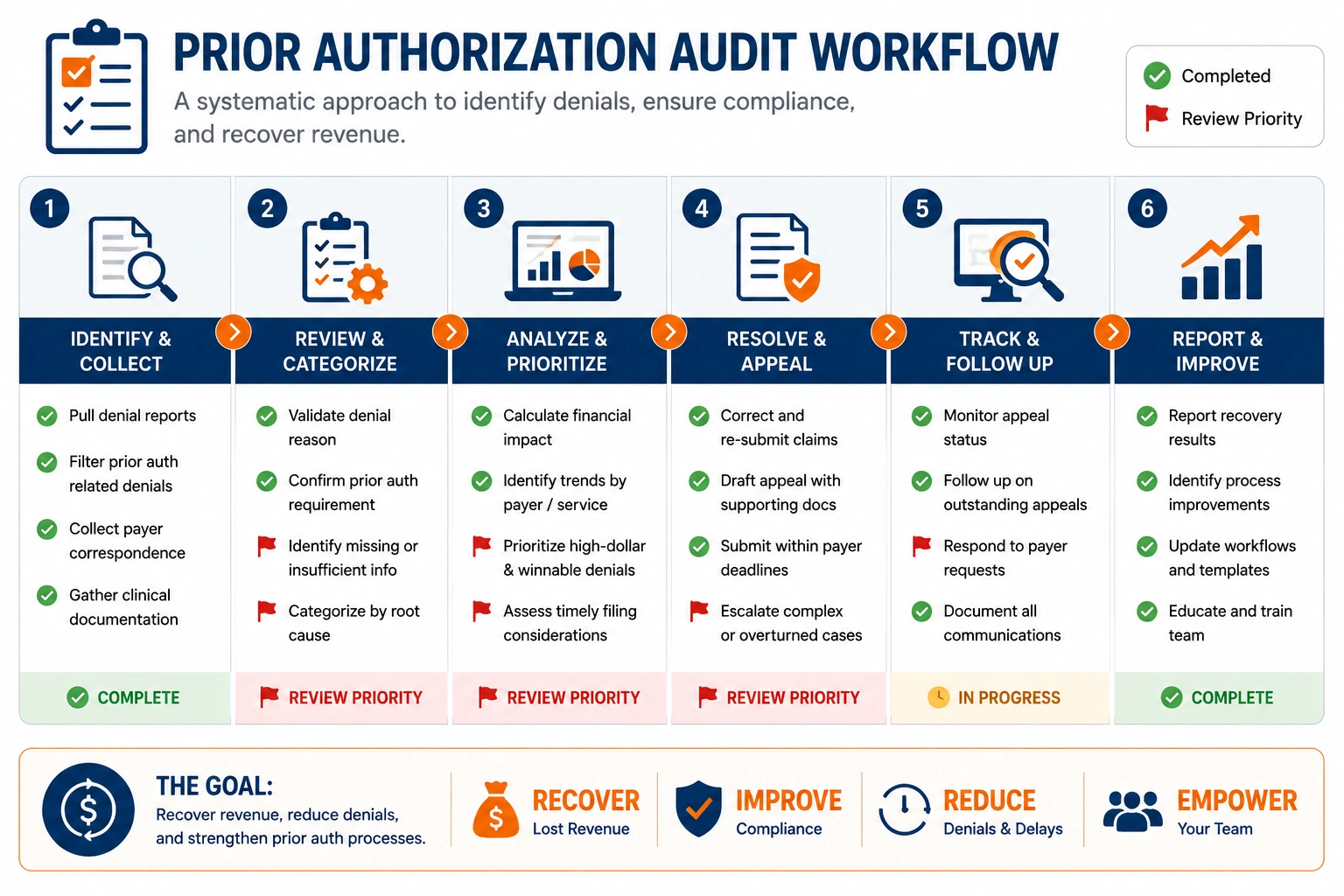
Conducting a Prior Authorization Audit
A structured prior authorization audit examines your last 90 to 180 days of prior auth submissions, denials, and appeals to identify:
- Which payers are generating the most denials and why
- Which CPT codes are triggering the most consistent rejections
- Whether denial reason types have shifted since January 2026
- Whether your team is meeting appeal deadlines consistently
This type of audit delivers some of the highest ROI of any revenue cycle activity — and most practices have never conducted one. Our medical coding services team ensures your CPT and ICD-10 coding is current and aligned with the latest payer prior authorization criteria, reducing auto-denials at the source.
Strategies Every Practice Should Implement Right Now
Strengthen Documentation Before Submission
Build a prior-authorization-specific documentation checklist into your pre-submission workflow. Every request should include complete medical necessity support, current ICD-10 and CPT code alignment, prior treatment history where step therapy applies, and physician sign-off on all supporting notes.
Adopt Electronic Prior Authorization (ePA) Workflows
Under CMS-0057-F, covered payers must now support FHIR-based Prior Authorization Support APIs. Check with your EHR vendor immediately about ePA integration status. Electronic prior authorization reduces manual errors, accelerates submission, and creates an automatic audit trail you can use for appeals and compliance documentation.
Track Appeal Deadlines Aggressively
Every denial should trigger an immediate calendar entry for the appeal deadline. This is not optional — missed appeal windows are permanent revenue losses. Build it into your standard denial management workflow, not as an afterthought, but as step one of your response protocol.
Monitor Gold Carding Eligibility by State
Assign a specific team member to track state gold carding laws on a quarterly basis and maintain a live log of which payers are actively applying exemptions. Physician approval rates shift. Laws get updated. Payer compliance status changes. This requires active monitoring, not a one-time assessment.
Invest in Dedicated Prior Authorization Staff or Partners
Prior authorization is a full-time function for any practice with moderate to high billing volume. If your team is managing prior auths alongside claims processing, coding, and denial management, things will fall through the cracks — and they will fall through in exactly the places that cost the most revenue.
How Outsourced Prior Authorization and Denial Management Protects Revenue
Proactive Denial Prevention
The highest-value strategy in prior authorization denial management is prevention — not recovery. An experienced outsourced partner submits requests with payer-specific documentation, monitors payer behavior trends, and flags high-risk submissions before they go out the door. That kind of upstream intervention prevents the rework cost entirely.
Faster, Better-Documented Appeals
When denials do happen, a specialized team responds faster and with appeal language precisely matched to the specific denial reason provided. Payer-specific framing and targeted clinical documentation are the difference between an overturn and an upheld denial — and that difference is measurable in dollars.
Payer-Specific Denial Tracking
A specialized revenue cycle partner tracks denial patterns across payers, procedures, and CPT codes continuously — and uses that data to improve your first-pass approval rate over time. This is data-driven prior authorization denial management at a level most in-house billing teams cannot sustain at scale.
How UtreatiBill Helps Practices Navigate the Prior Authorization Rule 2026
At UtreatiBill, our revenue cycle management team specializes in the specific challenges that CMS prior authorization 2026 requirements create for physician practices and specialty groups. Our services include:
- Prior authorization submission and tracking using ePA tools and payer-specific documentation protocols
- Denial management and appeals with specialty-specific appeal language and documented overturn tracking
- Monthly denial pattern reporting so your leadership always knows where revenue risk is concentrated
- Gold carding eligibility monitoring by payer and by state, updated quarterly
- Prior authorization audits identifying workflow gaps and quantifying revenue recovery opportunities
Whether your practice is single-specialty or managing a multi-provider group, UtreatiBill builds a prior authorization workflow that matches your payer mix, your specialty, and your volume.

Key Takeaways
- The prior authorization rule 2026 (CMS-0057-F) mandates 7-day standard and 72-hour urgent decision timelines, mandatory ePA implementation, and specific written denial reasons for all covered payers.
- Medicare Advantage plans represent the most complex and highest-volume prior authorization denial risk for most practices.
- Gold carding laws are active in more than 20 states, but payer enforcement gaps mean many qualifying physicians are still submitting unnecessary prior auths.
- The average claims rework cost per denied prior auth ranges from $43 to $196 — and most practices never appeal denials they could win.
- Monthly denial pattern monitoring and proactive documentation protocols deliver the highest ROI of any revenue cycle workflow investment.
- Outsourced prior authorization and denial management delivers measurable, sustainable revenue protection for practices that lack dedicated internal capacity.
Final Thoughts
The prior authorization rule 2026 creates real opportunities for practices that are ready to take advantage of them — faster payer decisions, better denial documentation, stronger appeal positions, and access to published payer performance data. But those advantages only materialize when your workflows, your documentation, and your denial management processes are aligned with the new environment.
Practices that have made those updates are already performing better. Practices that have not are accumulating preventable losses with each billing cycle that passes.
Your revenue is worth protecting. Your team deserves workflows, tools, and partners built for how prior authorization actually works in 2026.